Avicenna Journal of Clinical Microbiology and Infection. 12(4):231-234.
doi: 10.34172/ajcmi.3718
Brief Report
Evaluation of Antimicrobial Resistance and Frequency of bap Gene Among Acinetobacter baumannii Strains Isolated from Hospitalized Patients
Tahoora Mousavi Conceptualization, Methodology, Project administration, Resources, Validation, Writing – original draft, Writing – review & editing, 1 
Ali Shushtari Data curation, Investigation, Methodology, Validation, Writing – review & editing, 2
Elham Amiri Data curation, Investigation, Methodology, Validation, Writing – review & editing, 2
Mona Moshiri Formal analysis, Investigation, Methodology, Software, Validation, Writing – review & editing, 3
Mehrdad Gholami Conceptualization, Methodology, Project administration, Supervision, Validation, Writing – original draft, Writing – review & editing, 4, *
Author information:
1Molecular and Cell Biology Research Center, Hemoglobinopathy Institute, Faculty of Medicine, Mazandaran University of Medical Sciences, Sari, Iran
2Faculty of Medicine, Mazandaran University of Medical Sciences, Sari, Iran
3Department Immunology, Faculty of Medicine, Mazandaran University of Medical Sciences, Sari, Iran
4Department of Microbiology and Virology, Faculty of Medicine, Mazandaran University of Medical Sciences, Sari, Iran
Abstract
Background: Acinetobacter baumannii has emerged as a major cause of hospital-acquired infections, posing a significant threat, especially in critical care environments, with mortality rates reaching up to 35%. Its ability to form biofilm on various surfaces within healthcare settings further facilitates the transmission of infections, raising growing concerns. This study was designed to evaluate antimicrobial resistance and the frequency of bap gene among A. baumannii collected from hospitalized patients in Mazandaran Province.
Methods: This cross-sectional study was conducted on 100 clinical isolates of A. baumannii recovered from hospitalized patients. In accordance with Clinical and Laboratory Standards Institute (CLSI) guidelines, the antibiotic susceptibility profiles of the isolates were evaluated using the disk diffusion method. For colistin, the minimum inhibitory concentration (MIC) was determined by the broth microdilution method. The presence of the bap gene was assessed using conventional polymerase chain reaction (PCR).
Results: The findings revealed that A. baumannii strains demonstrated high resistance to several antibiotics, particularly carbapenems and cephalosporins, with limited effective treatment options. Notably, colistin, tobramycin, and gentamicin remained effective against these isolates. Importantly, the bap gene was detected in all A. baumannii isolates, highlighting its widespread prevalence.
Conclusion: This study highlights the substantial burden A. baumannii imposes on healthcare systems and patients due to its multidrug-resistant nature. The continued effectiveness of colistin, tobramycin, and gentamicin suggests the need to reconsider reliance on traditional antibiotics such as carbapenems. The prevalence of the bap gene underscores the urgency of addressing this virulent pathogen. These findings provide valuable insights for local healthcare strategies to combat A. baumannii infections and ultimately improve patient outcomes.
Keywords: Biofilm, Acinetobacter baumannii, bap gene
Copyright and License Information
© 2025 The Author(s); Published by Hamadan University of Medical Sciences.
This is an open-access article distributed under the terms of the Creative Commons Attribution License (
https://creativecommons.org/licenses/by/4.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Please cite this article as follows: Mousavi T, Shushtari A, Amiri E, Moshiri M, Gholami M. Evaluation of antimicrobial resistance and frequency of bap gene among acinetobacter baumannii strains isolated from hospitalized patients. Avicenna J Clin Microbiol Infect. 2025;12(4):231-234. doi:10.34172/ajcmi.3718
Introduction
Acinetobacter baumannii is a Gram-negative, aerobic bacterium with multidrug resistance (MDR) and multiple virulence factors. It possesses various antibiotic resistance mechanisms and causes serious problems in immunocompromised patients (1,2). Clinical isolates of A. baumannii can form biofilms on diverse surfaces. Notably, the emergence of biofilm-producing, antibiotic-resistant Gram-negative bacteria has become a growing concern, particularly among pathogens commonly encountered in healthcare environments (3).
A large 854-kDa protein known as biofilm-associated protein (BAP) is a key factor in biofilm production and adhesion to host cells (4). In recent years, only a few studies have examined the prevalence of the bap gene and its association with antibiotic-resistant A. baumannii strains.
Given the limited data on biofilm-forming ability and the prevalence of the biofilm-associated bap gene in A. baumannii, as well as its connection to antibiotic resistance in northern Iran, this study aimed to investigate the antibiotic susceptibility profiles and conduct a molecular evaluation of the bap gene in A. baumannii strains isolated from hospitalized patients.
Materials and Methods
Sample Collection
This cross-sectional study (February 2022 to June 2023), approved under the ethics code IR.MAZUMS.REC.1401.240, included 100 clinical samples collected from teaching hospitals in Sari County. The samples were obtained from pulmonary secretions, blood, wounds, urine, broncho-alveolar lavage (BAL), abscess, urinary catheters, pleural fluid, and cerebrospinal fluid (CSF).
Isolation and Identification of Acinetobacter baumannii Isolates
All samples were transferred to the microbiology laboratory and cultured on blood agar and MacConkey agar media. The inoculated plates were subsequently incubated at 37 °C for 24 hours to allow optimal bacterial growth. Preliminary identification of the isolates was performed using standard biochemical tests (5). Final confirmation of the A. baumannii strain was achieved through a standard polymerase chain reaction (PCR) assay targeting the bla-OXA-51 gene (bla-OXA-51-F: 5′-TAA TGC TTT GAT CGG CCT TG-3′, bla-OXA51-R: 5′-TGG ATT GCA CTT CAT CTT GG -3′) (6).
Antibiotic Susceptibility
Antibiotic susceptibility of all isolates was evaluated using the Kirby-Bauer disk diffusion method on Mueller-Hinton agar, following the 2021 Clinical and Laboratory Standards Institute (CLSI) guidelines. The susceptibility of the isolates was assessed using the following antimicrobial disks: gentamicin (30 µg), tetracycline (5 µg), imipenem (10 µg), tobramycin (10 µg), trimethoprim-sulfamethoxazole (30 µg), ceftazidime (30 µg), doripenem (30 µg), piperacillin-tazobactam (10 µg), ciprofloxacin (5 µg), cefepime (30 µg), piperacillin (30 µg), cefazolin (30 µg), amikacin (30 µg), and ampicillin (30 µg) (MAST, UK).
The minimum inhibitory concentration (MIC) for colistin against A. baumannii (0.25–128 μg/mL) was determined using the CLSI broth microdilution (BMD) method. MIC values were evaluated based on CLSI guidelines (7). Escherichia coli ATCC 25922 was employed as the standard reference strain for quality verification.
Identification of bla-OXA-51 Gene in Acinetobacter baumannii Isolates
In this study, the genome of 100 isolates was obtained using the boiling extraction method. PCR amplification was conducted under the following conditions: initial denaturation at 95 °C for five minutes, 30 cycles of 95 °C for 60 seconds, 50 °C for 50 seconds, 72°C for 60 seconds, followed by a final extension at 68°C for two minutes. DNA presence, concentration, and quality were assessed using agarose gel electrophoresis.
Polymerase Chain Reaction for Detection of the bap Gene
In the present study, the primers used for bap gene detection were: bap-F: 5′-TAGGGAGGGTACCAATGCAG-3′ and bap-R: 5′-TCATGATTTGATGCTGCAGCG-3′, applied in the PCR method (8).
Results
Descriptive Epidemiology
In the current study, 100 A. baumannii isolateswere collected from different clinical specimens, including pulmonary secretions (46%), blood (30%), wound (10%), urine (5%), BAL (3%), abscess (2%), urinary catheter (2%), pleural fluid (1%), and CSF (1%). Of the isolates identified as Acinetobacter spp. phenotypically, all were confirmed as A. baumannii using bla-OXA-51 primers, which yielded the expected 353 bp bands on agarose gel electrophoresis.
Antimicrobial Susceptibility Testing
The MIC results indicated that out of the 100 A. baumannii strains, 97 were susceptible and 3 were resistant to colistin. Susceptibility to other antibiotics was assessed using the standard disk diffusion assay. The detailed susceptibility profiles of other tested antibiotics are presented in Figure 1.
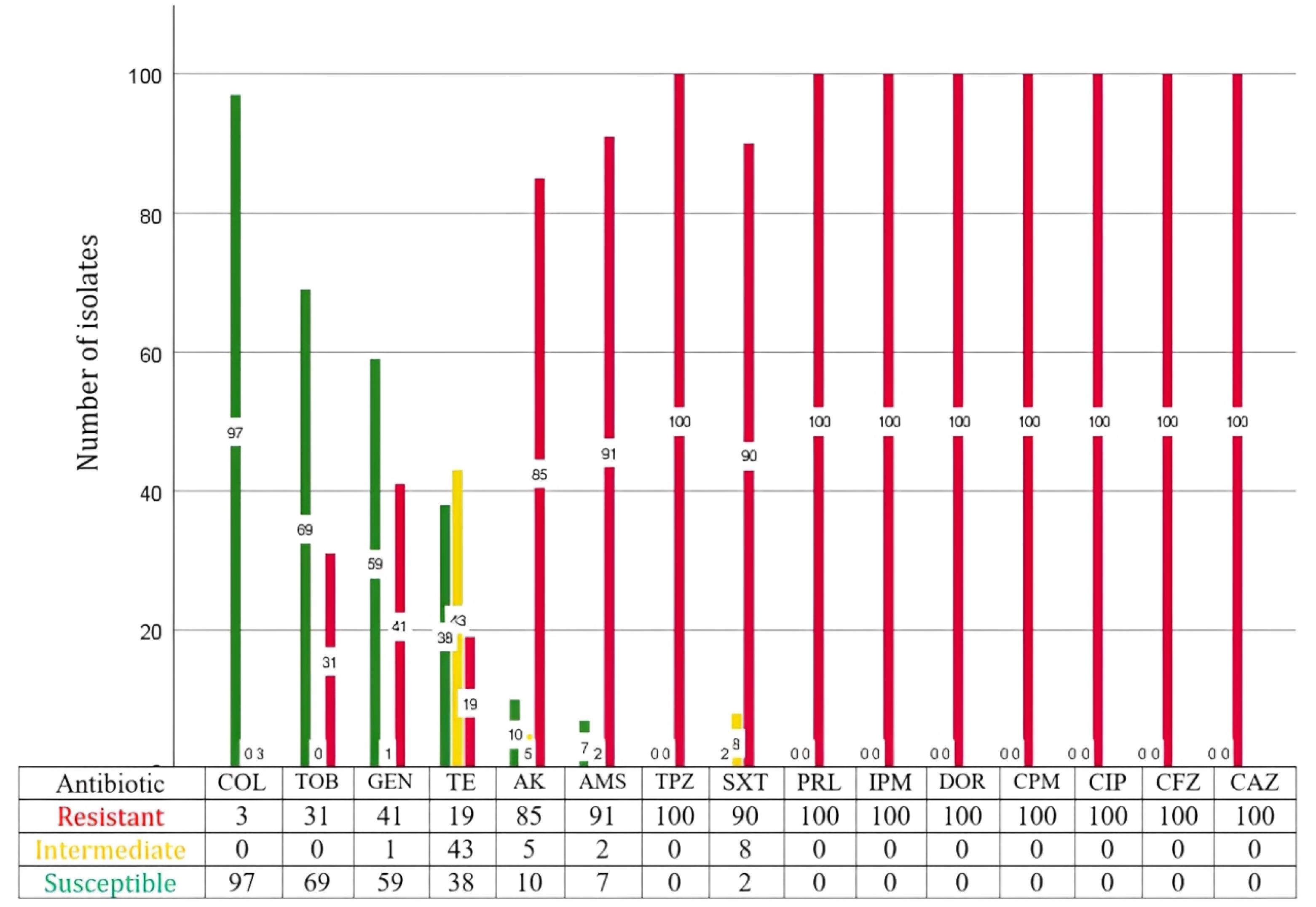
Figure 1.
Antibiotic Resistance Patterns of A. baumannii Isolates. Note: AK: Amikacine; AMS: Ampicillin-sulbactam; CAZ: Cefazolin; CFZ: Ceftazidime; CIP: Ciprofloxacine; COL: Colistin; CPM: Cefepime; DOR: Doripenem; GEN: Gentamicin; IPM: Imipenem; PRL: Piperacillin; SXT: Trimethoprim-sulfamethoxazole; TE: Tetracycline; TOB: Tobramycin; TPZ: Piperacillin-tazobactam
.
Antibiotic Resistance Patterns of A. baumannii Isolates. Note: AK: Amikacine; AMS: Ampicillin-sulbactam; CAZ: Cefazolin; CFZ: Ceftazidime; CIP: Ciprofloxacine; COL: Colistin; CPM: Cefepime; DOR: Doripenem; GEN: Gentamicin; IPM: Imipenem; PRL: Piperacillin; SXT: Trimethoprim-sulfamethoxazole; TE: Tetracycline; TOB: Tobramycin; TPZ: Piperacillin-tazobactam
Presence of bap
All isolates involved in this study carried the A. baumannii bap gene (Figure 2).
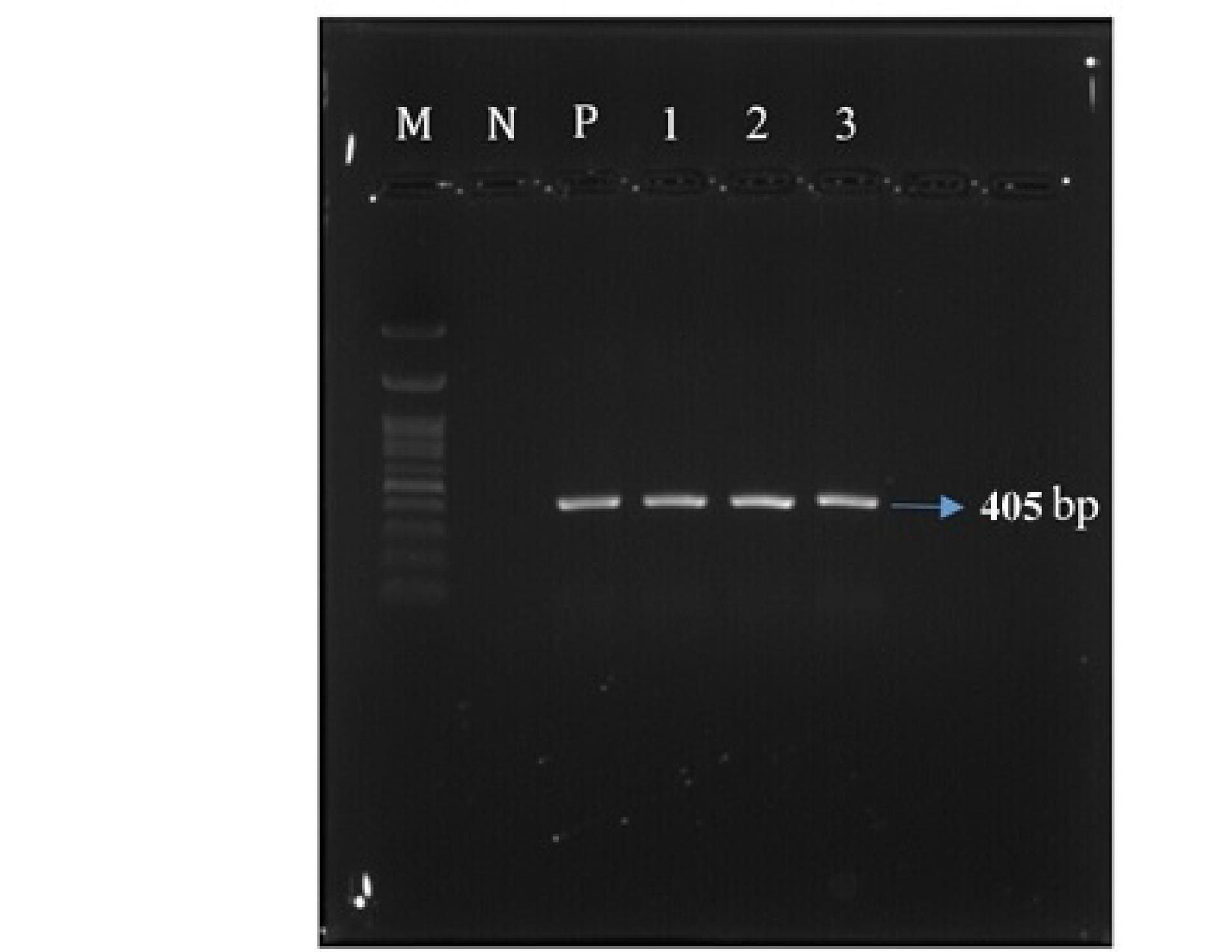
Figure 2.
PCR Image of Three A. baumannii Isolates (1,2,3) Showing 405 bp DNA Bands Representing the bap Gene. Note. M: DNA ladder; N: Negative control; P: Positive control
.
PCR Image of Three A. baumannii Isolates (1,2,3) Showing 405 bp DNA Bands Representing the bap Gene. Note. M: DNA ladder; N: Negative control; P: Positive control
Discussion
Over the past decade, A. baumannii has attracted increasing research interest as a major multidrug-resistant pathogen (9-11). Among its virulence-related genes, the bap gene has received considerable attention due to its critical role in biofilm formation, which enhances the persistence of A. baumannii in hospital environments where exposure to disinfectants is frequent (12,13).
In Iran, several studies have reported that the frequency of the bap gene among A. baumannii isolates ranges from 43% (14) to 100% (15). These high frequencies highlight the worldwide distribution and dissemination of this important virulence factor in A. baumannii strains. Similarly, in a study conducted on 53 A. baumannii clinical isolates collected from inpatients in Iraq, the frequency of the bap gene was reported to be 79% (16). The lowest frequency (43%) was reported by Zeighami et al, who examined 100 A. baumannii strains recovered from immunocompromised patients hospitalized in the intensive care units (ICUs) (14). The low frequencies observed in some studies may be due to geographical variations and differences in the source of isolates. For example, one of our reference hospitals (Shahid Zare) is a burn-specialized hospital where A. baumannii strains are exposed to extreme amounts of disinfectants and prophylactic antibiotics. The capacity of A. baumannii to form biofilms has been closely linked to the development of an MDR phenotype. Consistent with our observations, previous studies have reported a strong association between the presence of the bap gene and biofilm formation, as well as increased biofilm production in MDR isolates, highlighting the critical role of bap-related biofilms in enhancing antimicrobial resistance mechanisms in A. baumannii (17)
However, carbapenems (imipenem and doripenem) and cephalosporins (ceftazidime, cefepime, and cefazoline) were found to be completely ineffective against A. baumannii isolates, as none of the isolates exhibited susceptibility to these drugs. Interestingly, all isolates were resistant to imipenem and doripenem, as these drugs (Carbapenem family) are the first-line treatment for A. baumannii infections in many areas. Consistent with our findings, multiple studies have reported similarly high resistance rates of A. baumannii isolates to carbapenems (16,18-21).
These results suggest that carbapenems should be decommissioned as the drugs of choice for A. baumannii infections. In contrast, colistin and aminoglycosides (tobramycin and gentamicin) showed excellent activity against A. baumannii isolates. Several other studies have similarly reported a high susceptibility profile of A. baumannii isolates to colistin and aminoglycosides (16,18), supporting their use as potential therapeutic options for A. baumannii infections in Mazandaran province and northern Iran.
Conclusion
In conclusion, our study highlights the significant burden that A. baumannii imposes on healthcare systems and patients, primarily due to its MDR nature. We identified colistin, tobramycin, and gentamicin as effective treatment options, underscoring the need to reconsider reliance on traditional antibiotics such as carbapenems.
Acknowledgments
We thank the hospital staff for their assistance in collecting clinical isolates and preparing patient data.
Competing Interests
The authors declare no conflict of interests.
Ethical Approval
This study was approved by the Research Ethics Committees of Mazandaran University of Medical Sciences (MAZUMS) (Approval ID. IR.MAZUMS.REC.1401.240).
Funding
This work was funded by Mazandaran University of Medical Sciences, Sari, Iran (Grant No. 13945).
References
- Mittal KR, Jain N, Srivastava P, Jain CK. Multidrug-resistant Acinetobacter baumannii: an emerging aspect of new drug discovery. Recent Adv Antiinfect Drug Discov 2023; 18(1):29-41. doi: 10.2174/2772434417666220912120726 [Crossref] [ Google Scholar]
- Narjis MA, Mahdi MS. Isolation and identification of multi-drug resistance Acinetobacter baumannii isolated from clinical samples at Baghdad, Iraq. J Appl Nat Sci 2023; 15(2):663-71. doi: 10.31018/jans.v15i2.4499 [Crossref] [ Google Scholar]
- Pompilio A, Scribano D, Sarshar M, Di Bonaventura G, Palamara AT, Ambrosi C. Gram-negative bacteria holding together in a biofilm: the Acinetobacter baumannii Way. Microorganisms 2021; 9(7):1353. doi: 10.3390/microorganisms9071353 [Crossref] [ Google Scholar]
- Shukla SK, Rao TS. Targeting hydrophobicity in biofilm-associated protein (Bap) as a novel antibiofilm strategy against Staphylococcus aureus biofilm. Biophys Chem 2022; 289:106860. doi: 10.1016/j.bpc.2022.106860 [Crossref] [ Google Scholar]
- Gholami M, Hashemi A, Hakemi-Vala M, Goudarzi H, Hallajzadeh M. Efflux pump inhibitor phenylalanine-arginine Β-naphthylamide effect on the minimum inhibitory concentration of imipenem in Acinetobacter baumannii strains isolated from hospitalized patients in Shahid Motahari burn hospital, Tehran, Iran. Jundishapur J Microbiol 2015; 8(10):e19048. doi: 10.5812/jjm.19048 [Crossref] [ Google Scholar]
- Gholami M, Haghshenas M, Moshiri M, Razavi S, Pournajaf A, Irajian G. Frequency of 16S rRNA methylase and aminoglycoside-modifying enzyme genes among clinical isolates of Acinetobacter baumannii in Iran. Iran J Pathol 2017; 12(4):329-38. [ Google Scholar]
- Humphries R, Bobenchik AM, Hindler JA, Schuetz AN. Overview of changes to the clinical and laboratory standards institute performance standards for antimicrobial susceptibility testing, M100, 31st edition. J Clin Microbiol 2021; 59(12):e0021321. doi: 10.1128/jcm.00213-21 [Crossref] [ Google Scholar]
- Shahrokhi E, Hasani A, Ansarin K, Mikaili H, Hasani A, Aghazadeh M. Bacterial biofilm in ventilator-associated pneumonia: a clinical concern. J Res Med Dent Sci 2018; 6(4):46-51. [ Google Scholar]
- Liu X, Wu X, Tang J, Zhang L, Jia X. Trends and development in the antibiotic-resistance of Acinetobacter baumannii: a scientometric research study (1991-2019). Infect Drug Resist 2020; 13:3195-208. doi: 10.2147/idr.S264391 [Crossref] [ Google Scholar]
- Ibrahim S, Al-Saryi N, Al-Kadmy IMS, Aziz SN. Multidrug-resistant Acinetobacter baumannii as an emerging concern in hospitals. Mol Biol Rep 2021; 48(10):6987-98. doi: 10.1007/s11033-021-06690-6 [Crossref] [ Google Scholar]
- Gootz TD, Marra A. Acinetobacter baumannii: an emerging multidrug-resistant threat. Expert Rev Anti Infect Ther 2008; 6(3):309-25. doi: 10.1586/14787210.6.3.309 [Crossref] [ Google Scholar]
- Nor A’shimi M H, Alattraqchi AG, Mohd Rani F, NI AR, Ismail S, Abdullah FH. Biocide susceptibilities and biofilm-forming capacities of Acinetobacter baumannii clinical isolates from Malaysia. J Infect Dev Ctries 2019; 13(7):626-33. doi: 10.3855/jidc.11455 [Crossref] [ Google Scholar]
- Brossard KA, Campagnari AA. The Acinetobacter baumannii biofilm-associated protein plays a role in adherence to human epithelial cells. Infect Immun 2012; 80(1):228-33. doi: 10.1128/iai.05913-11 [Crossref] [ Google Scholar]
- Zeighami H, Valadkhani F, Shapouri R, Samadi E, Haghi F. Virulence characteristics of multidrug resistant biofilm forming Acinetobacter baumannii isolated from intensive care unit patients. BMC Infect Dis 2019; 19(1):629. doi: 10.1186/s12879-019-4272-0 [Crossref] [ Google Scholar]
- Aliramezani A, Soleimani M, Mazaheri Nezhad Fard R, Nojoomi F. Virulence determinants and biofilm formation of Acinetobacter baumannii isolated from hospitalized patients. Germs 2019; 9(3):148-53. doi: 10.18683/germs.2019.1171 [Crossref] [ Google Scholar]
- Saadulla SO, Muhammed SM. Detection of biofilm-related genes and antibiotic resistance in Acinetobacter baumannii isolated from clinical specimens. Biodiversitas 2023;24(3). doi: 10.13057/biodiv/d240356.
- Fallah A, Ahangarzadeh Rezaee M, Hasani A, Soroush Barhaghi MH, Samadi Kafil H. Frequency of bap and cpaA virulence genes in drug resistant clinical isolates of Acinetobacter baumannii and their role in biofilm formation. Iran J Basic Med Sci 2017; 20(8):849-55. doi: 10.22038/ijbms.2017.9105 [Crossref] [ Google Scholar]
- Maleki A, Kaviar VH, Koupaei M, Haddadi MH, Sadeghi Kalani B, Valadbeigi H. Molecular typing and antibiotic resistance patterns among clinical isolates of Acinetobacter baumannii recovered from burn patients in Tehran, Iran. Front Microbiol 2022; 13:994303. doi: 10.3389/fmicb.2022.994303 [Crossref] [ Google Scholar]
- Sadr M, Fahimzad SA, Karimi A, Fallah F, Armin S, Almasian Tehrani N. Antimicrobial resistance and molecular epidemiology of virulence genes among multi-drug resistant Acinetobacter baumannii clinical isolates in Iran. Gene Rep 2021; 24:101281. doi: 10.1016/j.genrep.2021.101281 [Crossref] [ Google Scholar]
- Derakhshan Sefidi M, Heidary L, Shams S. Prevalence of imipenem-resistant Acinetobacter baumannii isolates in Iran: a meta-analysis. Infect Epidemiol Microbiol 2021; 7(1):77-99. doi: 10.52547/iem.7.1.77 [Crossref] [ Google Scholar]
- Beigverdi R, Sattari-Maraji A, Emaneini M, Jabalameli F. Status of carbapenem-resistant Acinetobacter baumannii harboring carbapenemase: first systematic review and meta-analysis from Iran. Infect Genet Evol 2019; 73:433-43. doi: 10.1016/j.meegid.2019.06.008 [Crossref] [ Google Scholar]