Avicenna Journal of Clinical Microbiology and Infection. 12(3):121-128.
doi: 10.34172/ajcmi.3684
Original Article
A Large-Scale Retrospective Study on the Prevalence of COVID-19 and Urinary Bacterial Coinfections Among Hospitalized Patients in Salmas, Northwest Iran
Mohammad Sattari Tazehshahri 1  , Abbas Esmaeili Sani 2 , Aysan Helmi 3 , Marzieh Safari 1, *
, Abbas Esmaeili Sani 2 , Aysan Helmi 3 , Marzieh Safari 1, *
Author information:
1Department of Medical Laboratory Sciences, Urmia Branch, Islamic Azad University, Urmia, Iran
2Salmas Health Network, Urmia University of Medical Sciences, Urmia, Iran
3Salmas Khatam-al-Anbia Hospital, Urmia University of Medical Sciences, Urmia, Iran
Abstract
Background: The COVID-19 pandemic, caused by severe acute respiratory syndrome coronavirus 2, started with an outbreak of COVID-19 in Wuhan, China, in December 2019, resulting in millions of deaths in the following years. Bacterial coinfections and superinfections are concerns for patients with COVID-19. This study aimed to determine the mortality rate of COVID-19, its associated risk factors, and the bacterial isolates from urine samples of hospitalized patients suspected of having COVID-19 in Salmas, northwest Iran.
Methods: The data from 3,733 patients suspected of COVID-19 who were referred to Khatam Al-Anbiya hospital in Salmas, West Azerbaijan, Northwest Iran, from December 2019 to February 2024, were collected and analyzed in a retrospective study.
Results: Of the 3,733 patients, 2,172 (58.2%) tested positive for COVID-19, while 1,561 (41.8%) tested negative. Among those who tested positive, 1,210 were females (59.6%), and 962 were males (56.5%). The highest COVID-19 rate was observed in 2021 (72%), whereas the lowest rate was reported in 2024 (13.8%). Of the COVID-19-positive patients, 328 (15.1%) died, and the bacterial isolates from their urine samples included Escherichia coli (68.75%), which was the most prevalent isolate, followed by Klebsiella spp. (12.5%), coagulase-negative staphylococci spp. (10%), Enterobacter spp. (3.75%), nonhemolytic streptococci spp. (2.5%), Pseudomonas aeruginosa (1.25%), and Streptococcus beta-hemolytic spp. (1.25%).
Conclusion: Based on the results, the overall mortality rate of COVID-19 over five years was 15.1%. The most important risk factors for COVID-19-related death included older age, chronic kidney and lung diseases, diabetes mellitus, and male gender. Bacterial isolates from the urine samples of COVID-19 patients were E. coli, Klebsiella spp., coagulase-negative staphylococci spp., P. aeruginosa, Enterobacter spp., and non-hemolytic streptococci spp.
Keywords: COVID-19, Mortality, Urinary infection, Iran
Copyright and License Information
© 2025 The Author(s); Published by Hamadan University of Medical Sciences.
This is an open-access article distributed under the terms of the Creative Commons Attribution License (
https://creativecommons.org/licenses/by/4.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Please cite this article as follows: Sattari Tazehshahri M, Esmaeili Sani A, Helmi A, Safari M. A large-scale retrospective study on the prevalence of covid-19 and urinary bacterial coinfections among hospitalized patients in Salmas, northwest Iran. Avicenna J Clin Microbiol Infect. 2025;12(3):121-128. doi:10.34172/ajcmi.3684
Introduction
In late 2019, a cluster of pneumonia cases of unknown origin was reported in Wuhan, Hubei Province, China (1,2). It was caused by SARS-CoV-2, a coronavirus, which led to the disease known as COVID-19. The virus quickly spread worldwide, resulting in a pandemic (3). The virus primarily spreads through respiratory aerosols, which has caused most people and healthcare workers to wear personal protective equipment, especially face masks (4). The average incubation period is approximately 6.4 days (5), with common symptoms such as fever, cough, shortness of breath, muscle pain, and fatigue (5-7). It infected about 500 million people and caused over six million deaths by the end of March 2022. The pandemic was so severe that the World Health Organization declared it a Public Health Emergency of International Concern on January 30, 2020. In severe cases of COVID-19, viral pneumonia can occur, which may develop into a condition similar to bacterial sepsis called a “cytokine storm,” linked to multiple organ failure and higher inflammatory biomarkers (8). Bacterial infections associated with COVID-19 or other viral infections fall into two categories. Coinfections develop due to weakened immune systems, increased nasopharyngeal colonization, and damage to the respiratory tract mucosa, occurring simultaneously or shortly after COVID-19 or other viral symptoms. Superinfections, often healthcare-associated infections, show clinical signs and diagnostic features similar to other healthcare-associated infections and typically affect patients with severe COVID-19 who have undergone invasive procedures during hospitalization (9). Considering the existence of coinfections (10) and superinfections (11), studies have shown that patients with viral infections who are coinfected with other microorganisms face a higher mortality rate linked to respiratory viral infections (12). Bacterial co-infection occurs alongside viral infections, such as SARS, Middle East respiratory syndrome, influenza, and respiratory syncytial virus.
In patients with influenza, the estimated coinfection rate with bacteria ranges from 2% to 65%. The most common species responsible for these coinfections are Staphylococcus aureus and S. pneumoniae, occurring in 35% and 28% of cases, respectively. (8,13). In SARS, bacterial and/or fungal coinfection rates ranged from 1% to 43%, with S. pneumoniae and Staphylococcus spp. being the most commonly reported upon admission. Different studies report varying rates of bacterial coinfection among COVID-19 patients. Coagulase-negative Staphylococcus spp. and Enterococcus spp. are the most frequently detected bacterial infections in the bloodstream of COVID-19 patients. Additionally, methicillin-resistant S. aureus, Pseudomonas aeruginosa, Enterobacter spp., and Klebsiella spp. are prevalent pathogens isolated from individuals with ventilator-associated pneumonia in COVID-19 cases. Conversely, the typical sites of infection in community-acquired bacterial infections linked to COVID-19 include the urinary tract, with Escherichia coli and K. pneumoniae being prevalent (8), the respiratory tract (S. pneumoniae, Haemophilus influenzae, and S. aureus) (14), and skin and soft tissues (8). According to a report, the most common bacterial coinfections in COVID-19 patients are caused by the Enterobacter spp., followed by S. aureus. Among intensive care unit (ICU) patients, 37% experienced urinary coinfections, primarily caused by E. coli. Additionally, it has been reported that ICU patients who received at least one antibiotic during acute hospitalization developed secondary bacterial infections that required further antibiotic treatment (15).
Although treating COVID-19 patients with antimicrobial medications has proven to be ineffective, there are several reasons why antimicrobials are still prescribed; patients may exhibit symptoms that resemble bacterial or other virus-caused pneumonias, and there could be suspected or confirmed coinfections; moreover, protocols and existing healthcare frameworks might recommend the use of antimicrobials (16).
The estimated incubation period of COVID-19 is approximately 5.68 days. ICU admission lasts around 9.84 days, while recovery takes about 18.55 days. Death occurs within roughly 15.93 days. The pooled case fatality rate among confirmed COVID-19 patients is estimated to be 0.02 (17).
The current retrospective study aims to report the frequency of COVID-19 patients, including their demographics, symptoms, and bacterial coinfections, documented in Salmas, Northwest Iran.
Materials and Methods
Study Time and Region
This retrospective study analyzed recordings of patients suspected of having COVID-19 who were referred to Khatam Al-Anbiya hospital in Salmas, West Azerbaijan, northwest Iran, from December 2019 to February 2024.
Study Population and Analyses
The study included recordings of 3,733 patients, consisting of 2,030 (54.4%) females and 1,703 (45.6%) males. All available data were analyzed using SPSS software (IBM SPSS Statistics for Windows, Version 23.0. IBM Corporation, Armonk, NY), including COVID-19 test results, underlying medical conditions, demographics, symptoms, mortality, and prescribed medications.
Diagnosis of Coronavirus Disease 19
Nasal and/or throat swab samples were used for diagnosing COVID-19 by RNA extraction (ROJE, Iran) and real-time polymerase chain reaction (Pishtaz Teb, Iran) kits.
Urine Culture
First morning midstream urine samples and catheterized urine samples were taken from patients in the wards and the ICU, respectively.
Results
The recordings of 3,733 patients, including 2,030 (54.4%) females and 1,703 (45.6%) males, were analyzed. Clinical samples collected from COVID-19 patients included throat swabs (139, 3.7%), nasal swabs (11, 0.3%), and combined nasal and throat swabs (3,583, 96%). The mean age (standard deviation) of the studied population was 51.77 ± 26.37264 (SD), with females at 52.36 ± 25.90972 and males at 51.06 ± 26.90478 years. The number of patients was 34 (0.9%), 1014 (27.2%), 1634 (43.8%), 538 (14.4%), 296 (7.9%), and 217 (5.8%) in 2019, 2020, 2021, 2022, 2023, and 2024, respectively. The minimum age was less than 1 year, while the maximum age was 97. Of the 3,733 patients, 2,172 (58.2%) tested positive for COVID-19, while 1,561 (41.8%) tested negative. COVID-19 was positive in 1,210 females (59.6%) and 962 males (56.5%), the details of which are provided in Table 1.
Table 1.
COVID-19 Positivity Among Variables at the Reception of the Studied Population
|
Variable
|
|
COVID-19
|
Total
|
P
Value
|
OR
|
Positive (% in Rows)
(% in Columns
|
Negative (% in Rows)
(% in Columns)
|
| Gender |
Female |
1,210 (59.6%) |
820 (40.4%) |
2,030 |
0.054 |
1.135 |
| Male |
962 (56.5%) |
741 (43.5%) |
1,703 |
1 |
| Fever (above 38°) |
Yes |
470 (45.3%) |
567 (54.7%) |
1,037 |
< 0.001 |
1 |
| No |
1,702 (63.1%) |
994 (36.9%) |
2,696 |
2.066 |
| Registration date |
2019 |
12 (35.3%) |
22 (64.7%) |
34 |
< 0.001 |
- |
| 2020 |
691 (68.1%) |
323 (31.9%) |
1,014 |
| 2021 |
1,177 (72%) |
457 (28.0%) |
1,634 |
| 2022 |
206 (38.3%) |
332 (61.7%) |
538 |
| 2023 |
56 (18.9%) |
240 (81.1%) |
296 |
| 2024 |
30 (13.8%) |
187 (86.2%) |
217 |
| Sample type |
Throat swab |
70 (50.4%) |
69 (49.6%) |
139 |
0.022 |
- |
| Nasal swab |
3 (27.3%) |
8 (72.7%) |
11 |
| Nasal and throat swab |
2,016 (58.3%) |
1,444 (41.7%) |
3,460 |
COVID-19 positivity among patients without fever at reception was significantly higher (63.1%) compared to those with fever (45.3%), with an odds ratio of 2.066 (P< 0.001). The highest rate of COVID-19 was observed in 2021 (72%), followed by 2020 (68.1%), 2022 (38.3%), 2019 (35.3%), 2023 (18.9%), and 2024 (13.8%), with the difference being statistically significant (P < 0.001). The highest positive rate was found in nasal and throat swabs (58.3%), followed by throat swabs (50.4%) and nasal swabs (27.3%), respectively (P < 0.001, Table 1, Figure 1).
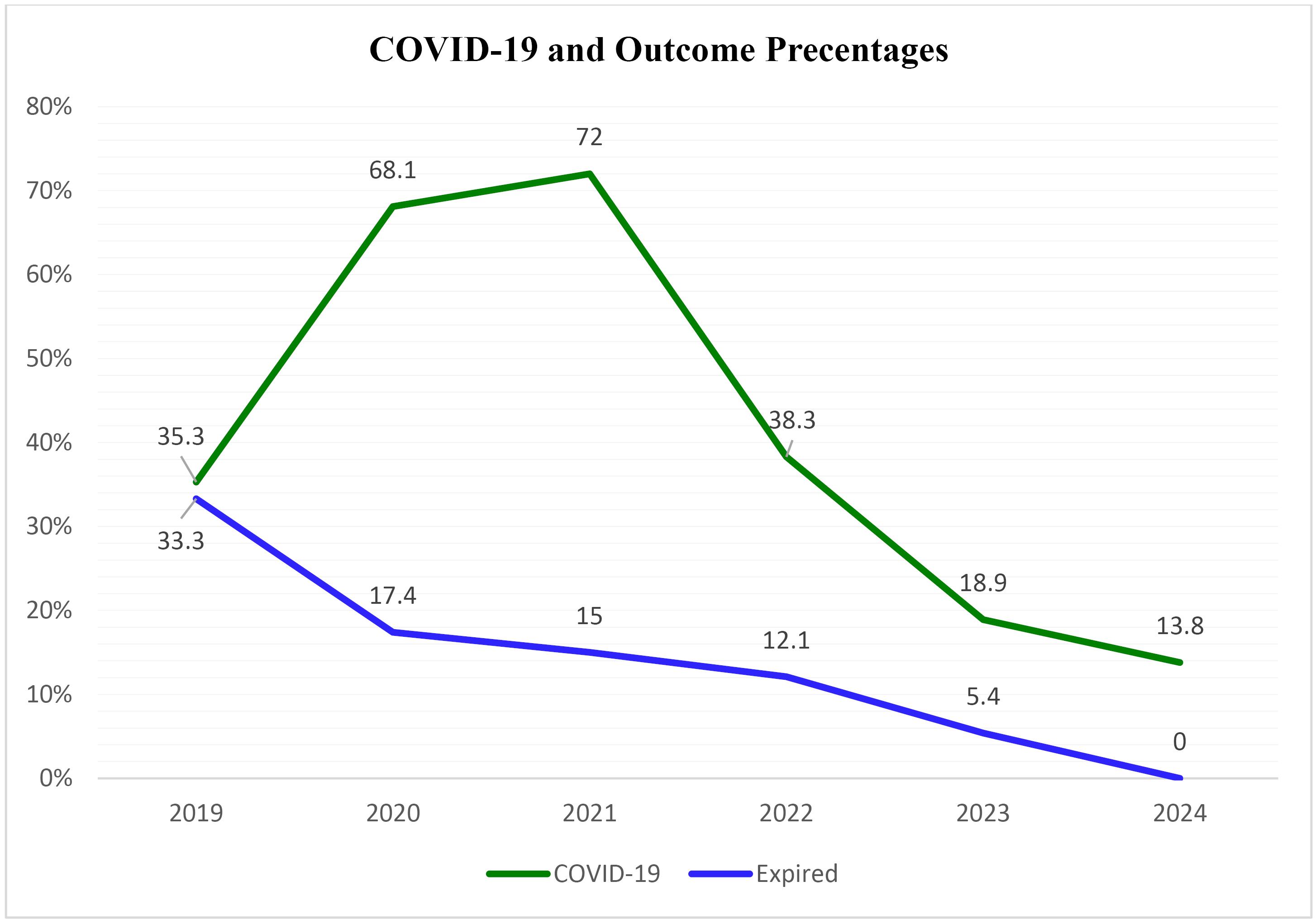
Figure 1.
The Trend of COVID-19 and the Death Rate of the Studied Patients During the Pandemic and Post-Pandemic Years
.
The Trend of COVID-19 and the Death Rate of the Studied Patients During the Pandemic and Post-Pandemic Years
The prevalence of COVID-19 was significantly higher in patients with dyspnea (77.9%), hemoptysis (70.6%), hypertension (63.2%), and diabetes mellitus (63.1%) compared to those without immunodeficiency (35.9%), chronic heart disease (50.6%), chronic lung disease (50.2%), chronic neurological disease (45.6%), seizures (45.6%), and non-pregnant women. The highest COVID-19 positivity was observed in the 40–60 age group (73.7%), followed by the 20–40 (66.7%), 60–80 (62.1%), > 80 (54.9%), and < 20 (21.0%) age groups. Among deceased patients, 65% were COVID-19 positive, while among discharged patients, 57.5% were COVID-19 positive, indicating a significant difference (P = 0.002). Other variables, such as chronic kidney disease (52.0%), chronic liver disease (41.7%), underlying diseases, such as malignancies (44.1%), and other medical histories (58.6%), demonstrated no significant difference in COVID-19 positivity (Table 2). Among COVID-19 positive patients, 328 (15.1%) died, while 1,832 (84.34%) were discharged (twenty patients were referred to other hospitals).
Table 2.
COVID-19 Positivity Rates Related to the Signs and Risk Factors of the studied Population
|
Variable
|
|
COVID-19
|
Total
|
P
|
OR
|
|
Positive (%)
|
Negative (%)
|
| Medical history |
Yes |
1,064 (58.6) |
752 (41.4) |
1,816 |
0.624 |
1.033 |
| No |
1,108 (57.8) |
809 (42.2) |
1,917 |
1 |
| Dyspnea |
Yes |
81 (77.9) |
23 (22.1) |
104 |
< 0.001 |
1 |
| No |
2,088 (57.7) |
1,532 (42.3) |
3,620 |
0.38 |
| Hemoptysis |
Yes |
422 (70.6) |
176 (29.4) |
598 |
< 0.001 |
1.893 |
| No |
1,747 (55.9) |
1,379 (44.1) |
3,126 |
1 |
| Hypertension HX |
Yes |
660 (63.2) |
384 (36.8) |
1,044 |
< 0.001 |
1.338 |
| No |
1,512 (56.2) |
1,177 (43.8) |
2,689 |
1 |
| Immunodeficiency disease HX |
Yes |
28 (35.9) |
50 (64.1) |
78 |
< 0.001 |
0.395 |
| No |
2,144 (58.7) |
1,511 (41.3) |
3,655 |
1 |
| Chronic heart disease HX |
Yes |
209 (50.6) |
204 (49.4) |
413 |
< 0.001 |
0.708 |
| No |
1,963 (59.1) |
1,357 (40.9) |
3,320 |
1 |
| Malignancy HX |
Yes |
15 (44.1) |
19 (55.9) |
34 |
0.095 |
0.564 |
| No |
2,157 (58.3) |
1,542 (41.7) |
3,699 |
1 |
| Chronic lung disease HX |
Yes |
107 (50.2) |
106 (49.8) |
213 |
0.015 |
0.711 |
| No |
2,065 (58.7) |
1,455 (41.3) |
3,520 |
1 |
| Chronic neurological disease HX |
Yes |
36 (45.6) |
43 (54.4) |
79 |
0.022 |
0.595 |
| No |
2,136 (58.5) |
1,518 (41.5) |
3,654 |
1 |
| Seizures HX |
Yes |
36 (45.6) |
43 (54.4) |
79 |
0.022 |
0.595 |
| No |
2,136 (58.5) |
1,518 (41.5) |
3,654 |
1 |
| Diabetes mellitus HX |
Yes |
413 (63.1) |
242 (36.9) |
655 |
0.005 |
1.28 |
| No |
1,759 (57.1) |
1,319 (42.9) |
3,078 |
1 |
| Chronic liver disease HX |
Yes |
5 (41.7) |
7 (58.3) |
12 |
0.245 |
0.512 |
| No |
2,167 (58.2) |
1,554 (41.8) |
3,721 |
1 |
| Pregnancy HX |
Yes |
34 (46.6) |
39 (53.4) |
73 |
0.042 |
0.621 |
| No |
2,138 (58.4) |
1,522 (41.6) |
3,660 |
1 |
| Chronic kidney disease HX |
Yes |
39 (52.0) |
36 (48.0) |
75 |
0.273 |
0.775 |
| No |
2,133 (58.3) |
1,525 (41.7) |
3,658 |
1 |
| Outcomes |
Expired |
328 (65.0) |
177 (35.0) |
505 |
0.002 |
1.37 |
| Discharged |
1,832 (57.5) |
1,354 (42.5) |
3,186 |
1 |
| Age group |
< 20 |
121 (21.0) |
456 (79.0) |
577 |
< 0.001 |
- |
| 20-40 |
339 (66.7) |
169 (33.3) |
508 |
| 40-60 |
658 (73.7) |
235 (26.3) |
893 |
| 60-80 |
776 (62.1) |
473 (37.9) |
1,249 |
| > 80 |
278 (54.9) |
228 (45.1) |
506 |
Note. OR: Odds ratio; HX: History.
The mean age of COVID-19 positive patients was 56.0244 ± 21.11860, significantly higher than that of negative patients, who averaged 45.8411 ± 31.35024 (P < 0.001). The mean age of COVID-19 positive patients who died was 68.8415 ± 15.88662, also significantly higher than the 53.7380 ± 21.08683 of those who survived and were discharged (P < 0.001), the data of which are presented in Table 3.
Table 3.
Mean Age in COVID-19 Positive and Negative Patients, and Among Expired and Discharged COVID-19 Positive Patients
|
|
COVID-19
|
N
|
Mean
|
Standard Deviation
|
Standard Error Mean
|
Mean Rank
|
P
Value
|
| Age |
Positive |
2,172 |
56.0244 |
21.11860 |
0.45314 |
1975.30 |
< 0.001 |
| Negative |
1,561 |
45.8411 |
31.35024 |
0.79349 |
1716.31 |
| Age (COVID-19 positive) |
Expired |
328 |
68.8415 |
15.88662 |
0.87719 |
1477.48 |
< 0.001 |
| Discharged |
1,832 |
53.7380 |
21.08683 |
0.49266 |
1009.42 |
The death rate from COVID-19 was significantly higher in males (17.3%), patients who had no fever (16%) upon admission, patients with diabetes mellitus (19.5%), those older than 80 (34.8%), and patients admitted in 2019 (33.3%). Moreover, it was noticeably higher in patients without dyspnea (15.5%), patients with hypertension (20.8%), those with chronic lung disease (29.9%), and patients with chronic kidney disease (35.9%) (Table 4, Figure 1).
Table 4.
values Estimated for Various Risk Factors and Demographic Variables in COVID-19 Positive Cases Among Expired and Discharged Patients
|
Variable
|
|
Outcomes (COVID-19 Positive Cases)
|
Total
|
P
Value
|
OR
|
|
Expired (%)
|
Discharged (%)
|
| Gender |
Female |
162 (13.5) |
1,040 (86.5) |
1,202 |
0.013 |
0.743 |
| Male |
166 (17.3) |
792 (82.7) |
958 |
1 |
| Urine bacterial culture |
Negative or not requested |
323 (15.3) |
1,794 (84.7) |
2,117 |
0.511 |
1.368 |
| Positive |
5 (11.6) |
38 (88.4) |
43 |
1 |
| Fever above 38 degrees |
Yes |
57 (12.2) |
411 (87.8) |
468 |
0.041 |
0.727 |
| No |
271 (16.0) |
1,421 (84.0) |
1,692 |
1 |
| Diabetes mellitus HX |
Yes |
80 (19.5) |
330 (80.5) |
410 |
0.007 |
1.468 |
| No |
248 (14.2) |
1,502 (85.8) |
1,750 |
1 |
| Age groups |
< 20 |
1 (0.8) |
118 (99.2) |
119 |
< 0.001 |
- |
| 20-40 |
20 (5.9) |
318 (94.1) |
338 |
| 40-60 |
58 (8.8) |
598 (91.2) |
656 |
| 60-80 |
153 (19.8) |
618 (80.2) |
771 |
| > 80 |
96 (34.8) |
180 (65.2) |
276 |
| Registration date |
2019 |
4 (33.3) |
8 (66.7) |
12 |
0.007 |
- |
| 2020 |
120 (17.4) |
571 (82.6) |
691 |
| 2021 |
176 (15.0) |
995 (85.0) |
1,171 |
| 2022 |
25 (12.3) |
1,78 (87.7) |
203 |
| 2023 |
3 (5.6) |
51 (94.4) |
54 |
| 2024 |
0 (0.0) |
29 (100.0) |
29 |
| Dyspnea |
Positive |
5 (6.2) |
76 (93.8) |
81 |
0.022 |
0.358 |
| Negative |
322 (15.5) |
1,754 (84.5) |
2,076 |
1 |
| Hypertension HX |
Yes |
137 (20.8) |
521 (79.2) |
658 |
< 0.001 |
1.805 |
| No |
191 (12.7) |
1,311 (87.3) |
1,502 |
1 |
| Chronic lung disease HX |
Yes |
32 (29.9) |
75 (70.1) |
107 |
< 0.001 |
2.533 |
| No |
296 (14.4) |
1,757 (85.6) |
2,053 |
1 |
| Chronic kidney disease HX |
Yes |
14 (35.9) |
25 (64.1) |
39 |
< 0.001 |
3.223 |
| No |
314 (14.8) |
1,807 (85.2) |
2,121 |
1 |
Note. OR: Odds ratio; HX: History.
Based on the results (Table 5), the most common complication of COVID-19 was bilateral infiltration with ground-glass opacification (98.1%), followed by bilateral infiltration (1.4%), secondary bacterial pneumonia (0.3%), primary viral pneumonia (0.1%), and bronchitis (0.05%).
Table 5.
Cross Tabulation of COVID-19 and Lung Complications in the Studied Patients
|
Complication
|
COVID-19
|
Total (%)
|
P
Value
|
|
Positive (%)
|
Negative (%)
|
| Bilateral infiltration |
30 (1.44) |
19 (1.45) |
49 (1.44) |
0.163 |
| Bilateral infiltration and ground-glass opacification |
2,042 (98.12) |
1,282 (97.86) |
3,324 (98) |
| Secondary bacterial pneumonia |
6 (0.28) |
2 (0.15) |
8 (0.23) |
| Primary viral pneumonia |
2 (0.096) |
0 (0.0) |
2 (0.058) |
| Bronchitis |
1 (0.048) |
3 (0.22) |
4 (0.11) |
| Cardiac arrest |
0 (0.0) |
2 (0.15) |
2 (0.058) |
| Hemorrhage |
0 (0.0) |
1 (0.076) |
1 (0.029) |
|
Total
|
2,081 (100) |
1,310 (100) |
3,391 (100) |
|
Table 6.
Bacterial Species Isolated From the Urine Culture of Patients Suspected of COVID-19 at the Physician’s Request
|
|
Bacterial Species
|
COVID-19
|
Total (%)
|
|
Positive (%)
|
Negative (%)
|
| Urine culture |
Escherichia coli
|
32 (74.41) |
23 (62.16) |
55 (68.75) |
|
Klebsiella spp. |
4 (9.30) |
6 (16.21) |
10 (12.5) |
| Coagulase-negative staphylococci spp. |
3 (6.97) |
5 (13.51) |
8 (10) |
|
Enterobacter spp. |
2 (4.65) |
1 (2.70) |
3 (3.75) |
| Nonhemolytic streptococci spp. |
1 (2.32) |
1 (2.70) |
2 (2.5) |
|
Pseudomonas aeruginosa |
1 (2.32) |
0 (0.0) |
1 (1.25) |
|
Streptococcus beta hemolytic spp. |
0 (0.0) |
1 (2.70) |
1 (1.25) |
|
Total
|
|
43 (100) |
37 (100) |
80 (100) |
Among hospitalized suspected COVID-19 patients, urine cultures were requested for some individuals. The results revealed that E. coli (68.75%) was the most common isolate, followed by Klebsiella spp. (12.5%), coagulase-negative staphylococci spp. (10%), Enterobacter spp. (3.75%), nonhemolytic streptococci spp. (2.5%), P. aeruginosa (1.25%), and Streptococcus beta-hemolytic spp. (1.25%).
Discussion
The recent pandemic caused by the SARS-CoV-2 virus has been one of the largest challenges for humanity in modern times and has overwhelmed the healthcare systems of almost all countries (16). The recordings of 3,733 patients suspected of having COVID-19 who were hospitalized at Khatam Al-Anbiya hospital in Salmas, Northwest Iran, were analyzed in the present study. Out of the 3,733 patients, 2,172 (58.2%) tested positive for COVID-19, while 1,561 (41.8%) tested negative. Among the COVID-19 positive patients, 328 (15.1%) passed away. The highest prevalence of COVID-19 was observed in 2021 (72%), while the lowest prevalence occurred in 2024 (13.8%) (Table 1). The highest mortality rate among COVID-19 positive patients was in 2019 (33.3%), with a decreasing trend afterward (Figure 1). The highest rate of COVID-19 was found in the age group of 40–60 years, but the highest mortality occurred in patients older than 80. Dyspnea was the most common symptom reported among COVID-19 patients compared to other symptoms. E. coli (74.41%) was the most frequently isolated bacterium from the urine cultures of COVID-19 patients.
The most widespread clinical features of COVID-19 in children were reported as fever (51%) and cough (41%). Typical imaging findings included normal images (41%) and ground-glass opacity (36%), while vomiting was observed in 33% of cases. Pediatric patients generally experience milder COVID-19 with uncommon clinical manifestations (18). Similarly, in adults, a systematic review reported that the major symptoms of COVID-19 were fever (83%) and cough (65.2%). Additionally, hypertension (18.5%) and cardiovascular disease (14.9%) were the most common comorbidities. Bilateral ground-glass opacities (66%) were identified as the most prevalent imaging finding. The pooled mortality rate was estimated at 6.6%, with males experiencing significantly higher mortality than females (OR 3.4) (19). Contrary to the results of the mentioned systematic review, in this study, 21.6% and 19.4% of hospitalized COVID-19 patients had a fever above 38 °C and hemoptysis, respectively, which are considerably lower. According to the records from the studied hospital, 49% of the hospitalized COVID-19 patients had one or more medical histories, with the most common comorbidities being hypertension (30.4%), followed by diabetes mellitus (19%), cardiovascular diseases (9.6%), and chronic lung disease (4.9%). The most common imaging finding was bilateral infiltration with ground-glass opacification in 98.2%. The overall mortality rate was 15.18% in hospitalized patients, which has continuously decreased since the highest in 2019. The highest recorded rates of COVID-19 cases and deaths occurred in the United States, India, Brazil, Russia, the United Kingdom, France, Italy, Spain, Turkey, Germany, Colombia, Argentina, Mexico, Poland, South Africa, Iran, Ukraine, Peru, Indonesia, and the Netherlands (5).
Bacterial infections associated with COVID-19 primarily occur in the community-acquired bacterial infections reported in the urinary tract (notably E. coli and K. pneumoniae) and the respiratory tract (including S. pneumoniae, Haemophilus influenzae, and S. aureus), as well as in the skin and soft tissues. Conversely, secondary bacterial infections can develop in bloodstream infections (mainly coagulase-negative Staphylococcus spp. and Enterococcus spp.) and ventilator-associated pneumonia (frequently caused by P. aeruginosa, methicillin-resistant S. aureus, Enterobacter spp., and Klebsiella spp.) (8). Similarly, in our study, E. coli and Klebsiella spp. were the most prevalent species of secondary bacterial infection isolated from the urine cultures of patients with COVID-19. However, other species were also isolated, including coagulase-negative staphylococci spp., Enterobacter spp., P. aeruginosa, and non-hemolytic streptococci spp.
The causes of coinfections and superinfections differ depending on the clinical situation (9). Coinfections in people with COVID-19 were examined in a 2020 meta-analysis. The report identified Mycoplasma pneumoniae as the main agent, while S. pneumoniae was notably absent (20), indicating potential selection or sample bias. Additionally, the study showed an overrepresentation of P. aeruginosa as a leading cause of community-acquired infections. This organism, often associated with healthcare-related infections, appeared more frequently than traditional community-acquired infection agents, such as S. pneumoniae and H. influenzae. This discrepancy likely suggests selection bias, difficulties in distinguishing between community-acquired and healthcare-acquired infections, or diagnostic practices, such as bronchoscopy in more critically ill patients (9).
Amerion et al examined the connection between COVID-19 outcomes and urine test results and found that features such as urine appearance, bacteria, casts, crystals, blood, protein, red and white blood cells, yeast cells, colony count, and positive bacterial growth in urine culture were strongly linked to mortality and ICU admission. They concluded that changes in urinary parameters in COVID-19 patients are related to disease outcomes. Therefore, careful monitoring of these urinary markers is recommended for early detection of potential complications (21). In the present study, there was no such relationship; this may be because not all patients received a urine test.
Limitations of the Study
Despite a large study population, the retrospective nature of the study introduces some limitations that may affect our findings. One issue was the urine culture data, which were not requested for all patients, and only positive cases were recorded, so statistical analysis could not explore potential relationships.
Conclusion
Based on the findings, the COVID-19 mortality rate over five years was 15.1%, indicating a decreasing trend, with the highest in 2019 and the lowest in 2024. The most significant risk factors for COVID-19-related death included older age, chronic kidney and lung diseases, diabetes mellitus, and male gender. Bacterial isolates from the urine of COVID-19 patients included E. coli, Klebsiella spp., coagulase-negative staphylococci spp., P. aeruginosa, Enterobacter spp., and non-hemolytic STREPTOCOCCI spp. Further research can explore respiratory viral infections and urinary bacterial coinfections to determine whether a relationship exists.
Acknowledgments
The authors would like to thank Khatam Al-Anbiya Hospital in Salmas, West Azerbaijan, Northwestern Iran, for their assistance and contributions.
Authors’ Contribution
A. H. conducted the laboratory work. In addition, M. S. T. and A. E. S. gathered the data. Finally, M. S. analyzed the data, wrote the main manuscript, and edited it.
Competing Interests
The authors declare that they have no conflict of interests.
Consent for Publication
Not applicable.
Data Availability Statement
Data will be available from the corresponding author upon reasonable request.
Ethical Approval
The present study was ethically approved by the Ethics Committee of the Urmia Branch, Islamic Azad University (ethical code IR.IAU.URMIA.REC.1402.122). Data, including test results, age, and gender of the patients, were obtained from the medical laboratory without revealing their names and reported as frequencies and percentages.
Funding
The current study received no financial support.
References
- Jin Y, Yang H, Ji W, Wu W, Chen S, Zhang W. Virology, epidemiology, pathogenesis, and control of COVID-19. Viruses 2020; 12(4):372. doi: 10.3390/v12040372 [Crossref] [ Google Scholar]
- Hu B, Guo H, Zhou P, Shi ZL. Characteristics of SARS-CoV-2 and COVID-19. Nat Rev Microbiol 2021; 19(3):141-54. doi: 10.1038/s41579-020-00459-7 [Crossref] [ Google Scholar]
- Umakanthan S, Sahu P, Ranade AV, Bukelo MM, Rao JS, Abrahao-Machado LF. Origin, transmission, diagnosis and management of coronavirus disease 2019 (COVID-19). Postgrad Med J 2020; 96(1142):753-8. doi: 10.1136/postgradmedj-2020-138234 [Crossref] [ Google Scholar]
- Ramaraj P, Super J, Doyle R, Aylwin C, Hettiaratchy S. Triaging of respiratory protective equipment on the assumed risk of SARS-CoV-2 aerosol exposure in patient-facing healthcare workers delivering secondary care: a rapid review. BMJ Open 2020; 10(10):e040321. doi: 10.1136/bmjopen-2020-040321 [Crossref] [ Google Scholar]
- Ochani R, Asad A, Yasmin F, Shaikh S, Khalid H, Batra S. COVID-19 pandemic: from origins to outcomes A comprehensive review of viral pathogenesis, clinical manifestations, diagnostic evaluation, and management. Infez Med 2021; 29(1):20-36. [ Google Scholar]
- Kordzadeh-Kermani E, Khalili H, Karimzadeh I. Pathogenesis, clinical manifestations and complications of coronavirus disease 2019 (COVID-19). Future Microbiol 2020; 15:1287-305. doi: 10.2217/fmb-2020-0110 [Crossref] [ Google Scholar]
- Singhal S, Kumar P, Singh S, Saha S, Dey AB. Clinical features and outcomes of COVID-19 in older adults: a systematic review and meta-analysis. BMC Geriatr 2021; 21(1):321. doi: 10.1186/s12877-021-02261-3 [Crossref] [ Google Scholar]
- Wu HY, Chang PH, Chen KY, Lin IF, Hsih WH, Tsai WL. Coronavirus disease 2019 (COVID-19) associated bacterial coinfection: incidence, diagnosis and treatment. J Microbiol Immunol Infect 2022; 55(6 Pt 1):985-92. doi: 10.1016/j.jmii.2022.09.006 [Crossref] [ Google Scholar]
- Grinbaum RS, Kiffer CR. Bacterial infections in COVID-19 patients: a review. Rev Assoc Med Bras (1992) 2021; 67(12):1863-8. doi: 10.1590/1806-9282.20210812 [Crossref] [ Google Scholar]
- McArdle AJ, Turkova A, Cunnington AJ. When do co-infections matter?. Curr Opin Infect Dis 2018; 31(3):209-15. doi: 10.1097/qco.0000000000000447 [Crossref] [ Google Scholar]
- Paget C, Trottein F. Mechanisms of bacterial superinfection post-influenza: a role for unconventional T cells. Front Immunol 2019; 10:336. doi: 10.3389/fimmu.2019.00336 [Crossref] [ Google Scholar]
- Mirzaei R, Goodarzi P, Asadi M, Soltani A, Aljanabi HA, Salimi Jeda A. Bacterial co-infections with SARS-CoV-2. IUBMB Life 2020; 72(10):2097-111. doi: 10.1002/iub.2356 [Crossref] [ Google Scholar]
- Klein EY, Monteforte B, Gupta A, Jiang W, May L, Hsieh YH. The frequency of influenza and bacterial coinfection: a systematic review and meta-analysis. Influenza Other Respir Viruses 2016; 10(5):394-403. doi: 10.1111/irv.12398 [Crossref] [ Google Scholar]
- Westblade LF, Simon MS, Satlin MJ. Bacterial coinfections in coronavirus disease 2019. Trends Microbiol 2021; 29(10):930-41. doi: 10.1016/j.tim.2021.03.018 [Crossref] [ Google Scholar]
- Santos AP, Gonçalves LC, Oliveira AC, Queiroz PH, Ito CR, Santos MO. Bacterial co-infection in patients with COVID-19 hospitalized (ICU and Not ICU): review and meta-analysis. Antibiotics (Basel) 2022; 11(7):894. doi: 10.3390/antibiotics11070894 [Crossref] [ Google Scholar]
- Kariyawasam RM, Julien DA, Jelinski DC, Larose SL, Rennert-May E, Conly JM. Antimicrobial resistance (AMR) in COVID-19 patients: a systematic review and meta-analysis (November 2019-June 2021). Antimicrob Resist Infect Control 2022; 11(1):45. doi: 10.1186/s13756-022-01085-z [Crossref] [ Google Scholar]
- Khalili M, Karamouzian M, Nasiri N, Javadi S, Mirzazadeh A, Sharifi H. Epidemiological characteristics of COVID-19: a systematic review and meta-analysis. Epidemiol Infect 2020; 148:e130. doi: 10.1017/s0950268820001430 [Crossref] [ Google Scholar]
- Cui X, Zhao Z, Zhang T, Guo W, Guo W, Zheng J. A systematic review and meta-analysis of children with coronavirus disease 2019 (COVID-19). J Med Virol 2021; 93(2):1057-69. doi: 10.1002/jmv.26398 [Crossref] [ Google Scholar]
- Nasiri MJ, Haddadi S, Tahvildari A, Farsi Y, Arbabi M, Hasanzadeh S. COVID-19 clinical characteristics, and sex-specific risk of mortality: systematic review and meta-analysis. Front Med (Lausanne) 2020; 7:459. doi: 10.3389/fmed.2020.00459 [Crossref] [ Google Scholar]
- Lansbury L, Lim B, Baskaran V, Lim WS. Co-infections in people with COVID-19: a systematic review and meta-analysis. J Infect 2020; 81(2):266-75. doi: 10.1016/j.jinf.2020.05.046 [Crossref] [ Google Scholar]
- Amerion N, Ebrahimi H, Goli S, Bagheri H, Rouhani M. The relationship between urine test findings and disease outcomes in hospitalized patients with COVID-19. Iran Journal of Nursing 2025; 38:E3092. doi: 10.32598/ijn.38.3092 [Crossref] [ Google Scholar]