Avicenna Journal of Clinical Microbiology and Infection. 12(4):204-219.
doi: 10.34172/ajcmi.3663
Review Article
From Omics to Artificial Intelligence: Revolutionizing Sepsis-Induced Acute Respiratory Distress Syndrome Management
Tamer A. Addissouky 1, 2, 3, * 
Author information:
1New Burg El-Arab Hospital, Ministry of Health, Alexandria, Egypt
2Department of Chemistry, Science Faculty, Menoufia University, Menoufia, Egypt
3American Society for Clinical Pathology (ASCP), Chicago, USA
Abstract
Background: Sepsis-induced acute respiratory distress syndrome (ARDS) represents a formidable challenge in critical care, marked by significant mortality and long-term morbidity among survivors. This study comprehensively reviewed the current advances in omics technologies, AI, and novel therapeutic approaches in sepsis-induced ARDS management.
Methods: The current literature on multi-omics approaches, advanced imaging modalities, biomarker development, and AI applications in sepsis-induced ARDS underwent investigation.
Results: Recent advances in high-throughput omics technologies (genomics, transcriptomics, proteomics, metabolomics, and epigenetics) have the enabled detailed dissection of the molecular and cellular pathways underlying sepsis-induced ARDS. These approaches have facilitated the discovery of key biomarkers in blood, urine, and exhaled breath condensate, offering promise for earlier diagnosis, precise risk stratification, and targeted intervention. Concurrently, developments in advanced imaging modalities (e.g., HRCT, MRI, and PET) have enhanced the visualization of pulmonary injury, improved disease monitoring, and informed therapeutic decision-making. Novel therapeutic modalities (i.e., nanoparticle-based drug delivery, lung-targeted and anti-inflammatory therapies, microbiome modulation, and extracorporeal life support) are expanding the therapeutic armamentarium. Furthermore, the integration of AI and ML into critical care workflows is transforming sepsis-induced ARDS management, enabling sophisticated predictive modeling, real-time clinical decision support, and the harnessing of big data analytics for precision medicine.
Conclusion: The synergy between omics technologies, advanced imaging, and AI is catalyzing a paradigm shift toward personalized medicine in sepsis-induced ARDS, with the potential to improve survival rates and long-term outcomes. Overall, these interdisciplinary innovations are reshaping the landscape of sepsis-induced ARDS by enabling more nuanced patient phenotyping, individualized therapy, and dynamic monitoring.
Keywords: Sepsis-induced acute respiratory distress syndrome, Biomarkers, Omics technologies, Novel therapeutics, Artificial intelligence, Personalized medicine
Copyright and License Information
© 2025 The Author(s); Published by Hamadan University of Medical Sciences.
This is an open-access article distributed under the terms of the Creative Commons Attribution License (
https://creativecommons.org/licenses/by/4.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Please cite this article as follows: Addissouky TA. From omics to artificial intelligence: revolutionizing sepsis-induced acute respiratory distress syndrome management. Avicenna J Clin Microbiol Infect. 2025;12(4):204-219. doi:10.34172/ajcmi.3663
Introduction
Sepsis-induced acute respiratory distress syndrome (ARDS) represents a critical health condition that is characterized by severe respiratory impairments caused by an uncontrolled inflammatory response to infection. This condition imposes a substantial burden on public health and adversely affects the quality of life of patients, with high mortality rates and persistent complications among survivors (1). Consequently, advancing research and innovation is essential to enhance outcomes for individuals impacted by sepsis-induced ARDS. Particularly, omics technologies have significantly transformed our comprehension of sepsis-induced ARDS by offering profound insights into its molecular underpinnings. Genomics, encompassing whole-genome sequencing and transcriptomics, facilitates the identification of genetic variations and gene expression profiles linked to ARDS onset and progression (2). In addition, proteomics allows for the quantitative examination of proteins and their post-translational modifications (PTMs), illuminating critical signaling pathways and disease markers. Metabolomics offers an integrative perspective on metabolic profiles and the synthesis of signaling molecules, thereby providing crucial data on dysregulated metabolic pathways. Moreover, epigenetic studies, including DNA methylation and histone modification analysis, deepen our understanding of gene expression regulation and cellular behavior in ARDS (3).
Advanced imaging modalities, such as high-resolution computed tomography (HRCT), magnetic resonance imaging (MRI), and positron emission tomography (PET), are indispensable in diagnosing and evaluating sepsis-induced ARDS (4). HRCT enables detailed visualization of lung structure and function, along with the early detection of lung injury (5). Further, MRI provides comprehensive insights into lung perfusion, gas exchange, and the presence of pulmonary edema and inflammation. Furthermore, PET imaging allows for the assessment of inflammatory activity and disease progression through measuring cellular metabolic processes (6). Moreover, the discovery and validation of novel biomarkers are critical in the context of sepsis-induced ARDS. Biomarkers derived from blood, urine, and exhaled breath condensate (EBC) hold potential for early diagnosis, risk stratification, and monitoring of treatment responses (7). However, significant barriers to translating these biomarkers into clinical practice remain, underscoring the need for innovative strategies to incorporate them into routine care (8). Multiplexed diagnostics (e.g., combinatorial biomarker detection, digital polymerase chain reaction, and next-generation sequencing) demonstrate promise in enhancing diagnostic precision and accuracy (9).
Emerging therapeutic approaches for sepsis-induced ARDS include lung-targeted therapies, anti-inflammatory interventions, vasoactive agents, and extracorporeal life-support techniques, such as extracorporeal membrane oxygenation (ECMO) and ventricular assist devices (VADs). Similarly, lung-targeted therapies, including inhalational corticosteroids, bronchodilators, and surfactant replacement therapy, aim to reduce inflammation while optimizing pulmonary function. Likewise, anti-inflammatory strategies involving corticosteroids, immunomodulatory drugs, and modulation of interleukins (IL), such as IL-6 and IL-10, offer potential for mitigating excessive immune responses. In addition, vasoactive agents, such as nitric oxide (NO) and prostacyclin analogs, aid in improving pulmonary circulation and oxygenation. It is noteworthy that ECMO and VADs provide critical life-saving support for patients experiencing severe respiratory and cardiac failure (10). The microbiome has emerged as a vital factor in the pathogenesis of sepsis-induced ARDS. Microbiome analysis, utilizing techniques such as 16S ribosomal RNA (rRNA) gene sequencing and shotgun metagenomics, elucidates the complex interactions between microbial communities and the host immune response. Further, microbiome-targeted interventions, including probiotics, prebiotics, fecal microbiota transplantation (FMT), and antibiotics targeting microbial virulence factors, offer promising avenues for modulating the microbiome and reducing ARDS severity (11). Nanoparticle (NP)-based drug delivery systems present several advantages, such as targeted delivery to the lungs, improved bioavailability, and minimized side effects. However, challenges like optimizing NP properties and ensuring their safety and efficacy must be addressed to fully exploit their potential for treating sepsis-induced ARDS (12).
The optimization of mechanical ventilation strategies remains crucial for improving ARDS patient outcomes. Advanced ventilation modalities, including adaptive support ventilation and non-invasive ventilation (NIV), provide tailored respiratory assistance to enhance lung function (13). Other approaches, such as adjusting positive end-expiratory pressure (PEEP) levels and managing tidal volume and plateau pressure, help mitigate lung injury. Furthermore, the open lung strategy, incorporating lung recruitment maneuvers and high-frequency oscillation ventilation, has demonstrated efficacy in improving ventilation-perfusion matching and preserving lung function (14). Big data analytics play a pivotal role in synthesizing data from diverse sources, such as electronic health records (EHRs), clinical trials, and omics studies (15). Personalized treatment strategies and improved patient outcomes can be achieved by analyzing these extensive datasets. Nonetheless, challenges regarding data quality, consistency, privacy, and security must be resolved to realize the full potential of big data analytics in critical care research (16). Virtual reality (VR) rehabilitation has shown promise in managing sepsis-induced ARDS by promoting early mobilization and exercise, thereby reducing complications. Nevertheless, barriers (e.g., cost, availability, and patient acceptance of VR rehabilitation programs) must be addressed for broader implementation (17). Personalized medicine, encompassing genomic profiling through whole-genome sequencing and targeted gene panels, in addition to pharmacogenomics for predicting drug responses and adverse effects, has the potential to revolutionize ARDS management. Tailored treatment plans and prevention strategies based on precision medicine principles can optimize individual outcomes (18). The integration of artificial intelligence (AI) and machine learning (ML) holds transformative potential in critical care. Likewise, predictive modeling for patient outcomes and disease progression informs decision-making and resource allocation (19). AI-driven clinical decision support systems (CDSSs) provide real-time monitoring and set up alerts for timely interventions, while natural language processing (NLP) enhances patient communication and clinical text analysis, thereby enabling valuable data insights (20).
Root Causes of Sepsis-Induced Acute Respiratory Distress Syndrome
Sepsis Pathogenesis
Pathogenesis describes the origin and progression of a disease, encompassing the sequence of events that culminate in its clinical manifestation. It involves investigating the underlying causes, mechanisms, and processes that drive the onset and evolution of a specific disease or condition. In the context of sepsis, pathogenesis refers to the intricate interaction between host and microbial factors that contribute to the development of the disease. Sepsis arises from an unregulated host response to an invading microorganism, which can initiate a cascade of pathological events, ultimately resulting in organ dysfunction and mortality (21). The pathogenesis of sepsis is multifaceted and progresses through distinct stages. It begins with the entry of microorganisms into the body via portals such as wounds or the respiratory tract. This invasion activates the body’s immune system, thereby triggering an inflammatory response characterized by redness, swelling, heat, and pain. The resulting inflammation can compromise the endothelium—the inner lining of blood vessels—by increasing its permeability and impairing blood flow. These effects contribute to tissue damage and the potential failure of critical organs (e.g., the kidneys, liver, and lungs) due to the unchecked inflammatory response (22). The systemic inflammatory response syndrome represents an extreme, body-wide inflammatory state that can escalate to multiple organ failure and death. As a severe and life-threatening complication of sepsis, septic shock is marked by critically low blood pressure, impaired oxygen delivery, and organ dysfunction despite adequate fluid resuscitation. Understanding the underlying mechanisms of sepsis pathogenesis has been pivotal in the development of therapeutic interventions, including the use of antimicrobials, vasopressors, and anti-inflammatory agents. Furthermore, advancements in early detection and management strategies have been instrumental in preventing the progression of sepsis to severe stages, such as septic shock and multi-organ failure (23).
Mechanisms of Sepsis-Induced Acute Respiratory Distress Syndrome
Sepsis-induced ARDS is a severe and frequently fatal complication of sepsis that is characterized by significant mortality. The systemic inflammation triggered by sepsis extends to the lungs, leading to damage to the alveolar-capillary membrane (24). This disruption compromises the barrier between airspaces and the bloodstream, allowing proteins and fluids to infiltrate the airspaces. Additionally, inflammation hampers lung function by limiting chest expansion, reducing lung compliance, and impairing oxygenation. Increased vascular permeability permits the entry of bacteria and inflammatory substances into the lungs, further exacerbating inflammation and tissue damage (25). A secondary consequence of sepsis (e.g., bacterial pneumonia) can amplify lung injury. Sepsis also induces a cytokine storm, characterized by excessive production of inflammatory cytokines, such as tumor necrosis factor-alpha (TNF-α), IL-1β, and IL-6, aggravating tissue destruction in the lungs. Oxidative stress, a hallmark of sepsis, causes an imbalance between the generation of reactive oxygen species and the antioxidant defenses of the body, leading to cellular injury and inflammation. Dysregulated NO production results in excessive NO levels, further intensifying lung damage. In addition, elevated platelet-activating factor contributes to inflammation, platelet aggregation, and vascular constriction, further impairing lung function (26). Genetic predispositions may also heighten susceptibility to ARDS in sepsis patients, as variations in certain immune and inflammatory response genes can influence disease severity. Accordingly, gaining insights into these mechanisms is essential for the development of targeted therapeutic interventions (27).
Alveolar injury in sepsis-induced ARDS may arise from direct or indirect damage caused by bacteria, viruses, or other harmful agents. Such damage activates alveolar macrophages, which release inflammatory mediators (e.g., TNF, IL-6, and IL-8), thereby recruiting neutrophils and monocytes to the site of injury. These activated neutrophils exacerbate tissue damage by releasing toxic substances, further compromising the alveolar barrier. This disruption results in the flooding of the interstitial and alveolar spaces with fluids and inflammatory cells. The inflammatory cascade is perpetuated by cytokines released from macrophages and neutrophils, thereby amplifying tissue damage and inflammation. Ultimately, this process leads to the destruction of alveolar structures and the accumulation of fluids due to the compromised barrier function. A thorough understanding of this inflammatory cascade is vital for devising therapeutic strategies aimed at halting the progression of inflammation and preserving alveolar integrity (9). Figure 1 illustrates the pathogenesis of sepsis-induced ARDS.
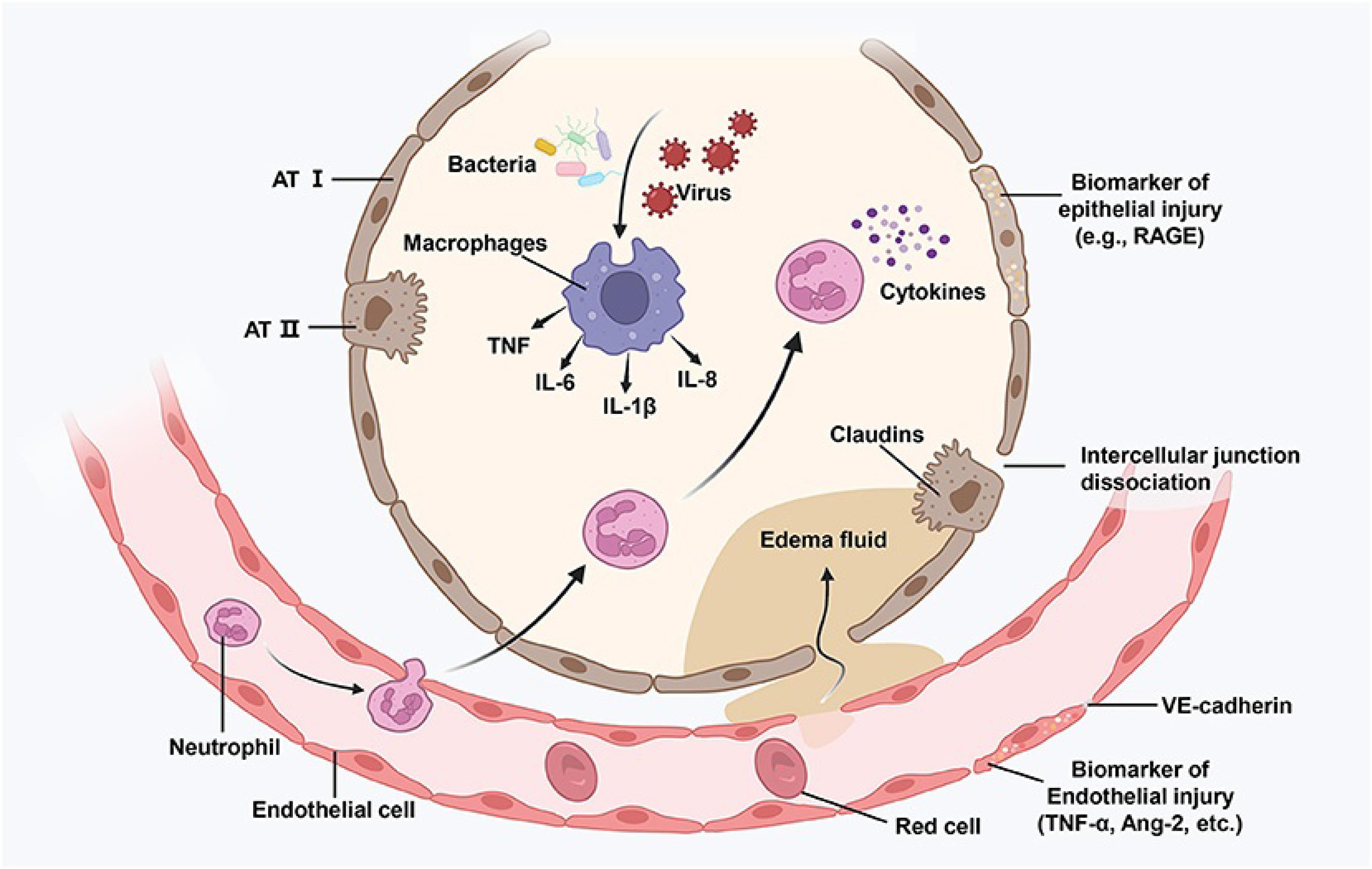
Figure 1.
Pathogenesis of Sepsis-Induced Acute Respiratory Distress Syndrome. Reprinted under the terms of the Creative Commons Attribution License (CC BY) (9)
.
Pathogenesis of Sepsis-Induced Acute Respiratory Distress Syndrome. Reprinted under the terms of the Creative Commons Attribution License (CC BY) (9)
Risk Factors
ARDS can result from a variety of direct and indirect insults to the lungs. As a severe systemic infection, sepsis is a leading cause of ARDS, primarily through immune-mediated inflammation that affects lung tissue. Moreover, pneumonia, another major contributor to ARDS, leads to inflammation and fluid accumulation within the alveoli, impairing gas exchange. Further, traumatic injuries (e.g., those caused by accidents or falls) can initiate ARDS through several mechanisms, such as shock and the release of fat emboli. Likewise, surgical procedures, particularly in individuals with preexisting lung conditions, can provoke ARDS due to the added stress on already compromised respiratory systems. Extensive burns affecting large areas of the skin can induce a systemic inflammatory response that damages the lungs. Similarly, smoke inhalation inflicts direct harm on lung tissue from heat, toxins, and oxygen deprivation. Additionally, exposure to hazardous chemicals (e.g., industrial agents or pesticides) causes caustic damage to the lungs, further increasing ARDS risk (28).
Furthermore, substance overdoses, particularly with respiratory depressants (e.g., opioids and benzodiazepines), are strongly associated with ARDS due to their suppression of normal breathing. Chronic alcohol consumption and smoking contribute to oxidative stress, which progressively damages lung tissue over time. Older adults, especially those with chronic health conditions, face a heightened risk of ARDS due to age-related immune system decline and structural changes in the lungs. Similarly, premature infants are particularly vulnerable to ARDS because of their underdeveloped and fragile lung architecture (29). Additionally, individuals with chronic lung diseases (e.g., chronic obstructive pulmonary disease and cystic fibrosis) have compromised respiratory function, making them more susceptible to ARDS. Organ failure, including heart, liver, or kidney dysfunction, can lead to fluid overload, resulting in pulmonary congestion. Malnutrition weakens the immune system, whereas obesity exacerbates conditions like diabetes and sleep apnea, thereby placing additional strain on the lungs. Pregnancy, especially in the third trimester, alters immune responses and increases ARDS risk. Immunocompromised individuals (e.g., those with human immunodeficiency virus/acquired immunodeficiency syndrome) are also more prone to lung injuries and ARDS. However, ARDS can occasionally develop in the absence of identifiable risk factors, highlighting the importance of prompt evaluation when respiratory distress occurs (30).
Omics Technologies
Sepsis-induced ARDS remains a significant challenge in critical care medicine, although omics technologies have substantially advanced the understanding of the pathophysiological mechanisms underlying this condition.
Genomics
Genomic research, particularly through whole-genome sequencing, has facilitated the identification of genetic variations linked to sepsis-induced ARDS. Variants in genes involved in immune responses, inflammation, and lung function have been associated with an increased risk of developing ARDS. For instance, Richa et al reported that individuals carrying a specific variant in the TLR4 gene were more likely to develop ARDS following sepsis (31). Additionally, transcriptomic analyses have unveiled changes in gene expression patterns in sepsis-induced ARDS patients. Research has shown that genes related to inflammation, immune responses, and apoptosis are differentially expressed in ARDS patients compared to healthy individuals. For example, the findings of one study revealed heightened expression of pro-inflammatory genes (e.g., NF- κB and IL-1β), along with reduced expression of anti-inflammatory genes (e.g., IL-10) in ARDS patients (32). Furthermore, integrative genomics approaches have clarified the relationship between genetic variations and gene expression changes in sepsis-induced ARDS. One such study identified variants in the IL-6 gene that were associated with increased gene expression and elevated serum IL-6 levels in ARDS patients (33).
Proteomics
Quantitative proteomics has enabled the identification of protein abundance changes and PTMs in sepsis-induced ARDS. In addition, proteomic studies have uncovered dysregulated proteins involved in inflammation, oxidative stress, and cell signaling in ARDS patients (34). For example, Gong et al identified elevated levels of pro-inflammatory cytokines (e.g., TNF-α and IL-1β), coupled with reduced levels of antioxidant proteins (e.g., superoxide dismutase) in ARDS patients (35). PTMs, which regulate protein function and activity, have also been investigated in the context of sepsis-induced ARDS (36). Yang et al reported dysregulated PTMs in proteins involved in inflammation, cell signaling, and lung function (37). For instance, Juanes-Velasco et al demonstrated increased levels of phosphorylated signal transducer and activator of transcription 3 (a transcription factor linked to inflammation) and decreased levels of acetylated histone H3 (a marker of chromatin relaxation) in ARDS patients (38).
Metabolomics
Metabolomic analyses have provided valuable insights into the metabolic disruptions that occur in sepsis-induced ARDS (Table 1). Alterations have been observed in metabolites associated with energy, amino acid, and lipid metabolism (39). For example, McClintock et al reported decreased glucose levels and elevated lactate levels in ARDS patients, suggesting impaired glucose metabolism (40). Likewise, Tian et al used metabolomics to explore the biogenesis and metabolism of signaling molecules in sepsis-induced ARDS and found changes in neurotransmitter, hormone, and inflammatory mediator metabolism (41). For instance, Li et al concluded that ARDS patients exhibited increased levels of prostaglandin E2 (a pro-inflammatory mediator) and decreased levels of dopamine (a neurotransmitter involved in vasodilation) (42).
Table 1.
Analytical Techniques in Proteomics and Metabolomics for Sepsis-Induced ARDS Research
|
Omics Field
|
Analytical Techniques
|
Principle and Strengths
|
Main Contributions
|
Key Findings/Applications
|
References
|
| Proteomics |
Liquid chromatography–tandem mass spectrometry (LC-MS/MS) |
- Separation of peptides/proteins by liquid chromatography, followed by identification and quantification via tandem mass spectrometry.
- High sensitivity and specificity for protein profiling and PTMs. |
- Quantitative and qualitative profiling of protein abundance
- Identification of PTMs (e.g., phosphorylation and acetylation)
- Discovery of disease biomarkers |
- Elevated pro-inflammatory cytokines (e.g., TNF-α and IL-1β)
- Alterations in antioxidant proteins (e.g., superoxide dismutase)
- PTMs, such as increased phosphorylated signal transducer and activator of transcription 3 and decreased acetylated histone H3 |
(34-36) |
|
|
Two-dimensional difference gel electrophoresis |
- Differential labeling of protein samples with fluorescent dyes, separation by isoelectric focusing and SDS-PAGE
- Quantitative comparison of protein spots |
- Comparative analysis of protein expression between conditions
- PTM analysis |
- Identification of dysregulated proteins and PTMs associated with ARDS progression |
(36,37) |
|
|
Matrix-assisted laser desorption/ionization-time of flight |
Rapid ionization and mass analysis of proteins/peptides from tissue or serum samples with minimal preparation. |
- High-throughput protein profiling
- Identification of protein biomarkers |
- Discrimination between healthy and ARDS patient proteomes |
(38) |
| Metabolomics |
LC-MS |
Separation of small molecules by LC, detection by MS
Suitable for a broad range of metabolites, including polar and non-polar compounds |
- Comprehensive profiling of metabolites
- Biomarker discovery
- Pathway elucidation |
- Detection of energy metabolism alterations: decreased glucose and increased lactate in ARDS
- Changes in amino acid and lipid profiles |
(39,40) |
|
|
LC-MS/MS (targeted and untargeted) |
Tandem MS allows for structural elucidation and quantification of targeted or global metabolite sets |
- Targeted quantitation of known metabolites
- Untargeted discovery of novel metabolic changes |
- Identification of metabolic pathways dysregulated in ARDS, such as increased prostaglandin E2 and decreased dopamine |
(3,41,42) |
|
|
Gas chromatography–mass spectrometry (GC-MS) |
Volatile and semi-volatile metabolites are separated by GC and detected by MS
Excellent for organic acids, fatty acids, and volatile organic compounds |
- Profiling of volatile metabolites (e.g., in EBC)
- Quantification of organic acids |
- Elevated levels of volatile organic compounds and oxidative stress markers in ARDS patients’ breath and fluids |
(40,43) |
|
|
Nuclear magnetic resonance spectroscopy |
- Non-destructive, quantitative analysis of metabolites based on magnetic properties of atomic nuclei
- Highly reproducible |
- Quantitative analysis of metabolite concentrations
- Structural elucidation |
- Identification of metabolic fingerprints distinguishing ARDS from controls
- Validation of targeted biomarker candidates |
(39) |
Note. ARDS: Acute respiratory distress syndrome; PTM:Post-translational modifications; TNF-α: Tumor necrosis factor-alpha; IL: Interleukin; SDS-PAGE: Sodium dodecyl sulfate polyacrylamide gel electrophoresis; EBC: exhaled breath condensate.
Epigenetics
Epigenetic mechanisms (e.g., histone modifications) play a critical role in regulating gene expression by altering chromatin structure, thereby influencing its accessibility to transcription factors, as presented in Table 2 (43). Some studies investigated histone modification changes in sepsis-induced ARDS (44). For example, Mailem and Tayo observed elevated levels of histone H3 lysine 9 trimethylation (H3K9me3), a marker of repressive chromatin, in the lung tissues of ARDS patients compared to healthy individuals. This increase in H3K9me3 was suggested to contribute to the silencing of genes involved in lung repair and regeneration (45). DNA methylation, another key epigenetic mechanism, involves the addition of methyl groups to cytosine residues in CpG dinucleotides and regulates gene expression. Altered DNA methylation patterns have been observed in sepsis-induced ARDS (46). For instance, Vanhorebeek and Van den Berghe reported increased DNA methylation at the promoter region of the IL-8 gene, which encodes a potent neutrophil chemoattractant. This hypermethylation was hypothesized to have a role in the overproduction of IL-8, thereby exacerbating lung injury in ARDS patients (47).
Table 2.
Omics Technologies in Sepsis-Induced ARDS Research: Techniques, Contributions, and Key Findings
|
Omics Technology
|
Key Techniques
|
Main Contributions to Sepsis-Induced ARDS Research
|
Examples of Findings
|
| Genomics |
- Whole-genome sequencing
- Transcriptomics - Integrative genomics |
- Identification of genetic variants associated with ARDS susceptibility
- Analysis of gene expression patterns
- Understanding gene-environment interactions |
- TLR4 gene variant associated with increased ARDS risk
- Increased expression of pro-inflammatory genes (NF-κB and IL-1β)
- Decreased expression of anti-inflammatory genes (IL-10) |
| Proteomics |
- Quantitative proteomics
- PTMs analysis |
- Measurement of protein abundance changes
- Identification of dysregulated proteins
- Analysis of protein modifications |
- Increased levels of pro-inflammatory cytokines (TNF-α and IL-1β)
- Decreased levels of antioxidant proteins (superoxide dismutase)
- Increased phosphorylation of signal transducer and activator of transcription 3
- Decreased acetylation of histone H3 |
| Metabolomics |
- Metabolite profiling
- Signaling molecule analysis |
- Identification of metabolic alterations
- Analysis of signaling molecule biogenesis and metabolism |
- Decreased glucose levels and increased lactate levels
- Increased prostaglandin E2 levels
- Decreased dopamine levels |
| Epigenetics |
- Histone modification analysis
- DNA methylation profiling |
- Investigation of chromatin structure changes
- Analysis of DNA methylation patterns |
- Increased histone H3 lysine 9 trimethylation in lung tissue
- Increased DNA methylation at the IL-8 gene promoter |
Note. ARDS: Acute respiratory distress syndrome; TLR4: Toll-like receptor 4; IL: Interleukin; TNF-α: Tumor necrosis factor-alpha; PTMs, post-translational modifications.
Advanced Imaging Techniques
These techniques are essential for diagnosing and managing sepsis-induced ARDS. These modalities provide detailed insights into lung structure, function, and pathophysiology, aiding in early detection, severity assessment, and treatment monitoring.
High-Resolution Computed Tomography
HRCT is a non-invasive imaging method that generates high-resolution images of lung parenchyma, thereby enabling detailed evaluation of lung structure and function. This method is widely used in diagnosing and monitoring sepsis-induced ARDS (48). Studies have highlighted the value of HRCT in identifying early lung injury. For example, research published in Radiology demonstrated that HRCT could detect subtle lung architectural changes (e.g., alveolar consolidation and ground-glass opacities) even before the clinical symptoms of respiratory failure become apparent. Similarly, Han et al revealed that HRCT could identify regions of the lung with impaired ventilation-perfusion matching, a key factor in ARDS pathogenesis (49). Additionally, HRCT provides information on lung function, including parameters like lung volume, air trapping, and gas diffusion. Likewise, Lee reported a strong correlation between HRCT-derived measures of lung volume and the partial pressure of arterial oxygen/fraction of inspired oxygen (PaO2/FiO2) ratio (an indicator of oxygenation status) in patients with sepsis-induced ARDS (50).
Magnetic Resonance Imaging
MRI uses magnetic fields and radio waves to produce detailed images of internal organs. This method has become increasingly valuable in studying lung diseases, including sepsis-induced ARDS. One of the key advantages of MRI is its ability to assess lung perfusion and gas exchange. Osawa et al concluded that MRI could accurately quantify lung blood flow and gas exchange, offering critical insights into sepsis-induced ARDS pathophysiology. MRI can also detect complications such as pulmonary edema and inflammation, which are common in ARDS (51). Furthermore, MRI provides functional information about lung tissue. For instance, Ge et al found that MRI-derived metrics of lung stiffness and strain were significantly correlated with the PaO2/FiO2 ratio, suggesting that MRI could be a useful tool for monitoring disease severity and treatment response in sepsis-induced ARDS (52).
Positron Emission Tomography Imaging
PET, a nuclear medicine imaging technique, visualizes cellular metabolic activity. It has been applied for studying inflammatory conditions, including sepsis-induced ARDS (53). PET imaging provides valuable insights into inflammatory responses and disease progression in ARDS. For example, some researchers used PET imaging to examine inflammation dynamics in mice with sepsis-induced ARDS, demonstrating its ability to monitor changes in inflammatory activity over time and to identify molecular targets for therapy (54,55). PET imaging is also useful for assessing treatment efficacy. A number of scholars evaluated PET imaging to monitor corticosteroid therapy in sepsis-induced ARDS patients, finding that it could detect changes in inflammatory activity and help optimize drug dosages and treatment timing (56,57).
Biomarker Development
Identification of Novel Biomarkers
Blood and Urinary Biomarkers
Blood and urinary biomarkers have shown promise for the early detection and monitoring of sepsis-induced ARDS. These biomarkers include proteins, cytokines, chemokines, and metabolites altered during systemic inflammation and organ dysfunction (8). For instance, elevated levels of IL-6, TNF-α, and neutrophil gelatinase-associated lipocalin (NGAL) have been linked to sepsis-induced ARDS (58).
Exhaled Breath Condensate Biomarkers
EBC contains volatile and non-volatile compounds that reflect lung physiology and can potentially diagnose and monitor respiratory diseases, including sepsis-induced ARDS. Research has shown that the concentrations of NO, carbon monoxide, and hydrogen peroxide in EBC are altered in ARDS, highlighting their potential as biomarkers (59).
Validation and Clinical Implementation
While promising, translating biomarkers into clinical practice faces challenges, including (1) standardizing sample collection, storage, and analysis, (2) establishing reference ranges, and (3) addressing confounding variables (60). Cost-effectiveness, availability, and user-friendly assays are also critical for widespread adoption (61). Strategies to overcome these barriers include multicenter validation studies, analytical method harmonization, and biomarker incorporation into EHRs. Point-of-care testing and minimally invasive sampling methods can further enhance feasibility while reducing costs (62).
Multiplexed Diagnostics
Multiplexed diagnostic platforms enable simultaneous measurement of multiple biomarkers, thereby improving diagnostic accuracy and providing a more comprehensive understanding of disease mechanisms. For example, a multiplex immunoassay panel measuring IL-6, TNF-α, and NGAL has been developed to differentiate sepsis-induced ARDS from other ARDS causes (63). Emerging technologies (e.g., digital polymerase chain reaction and next-generation sequencing) allow highly sensitive detection of nucleic acid biomarkers. These tools have identified novel genetic markers associated with sepsis susceptibility and outcomes. Nonetheless, further research is required to assess their clinical utility (64).
Novel Therapeutic Approaches
Lung-Targeted Therapies
Inhalational corticosteroids, which have anti-inflammatory properties, are being investigated for sepsis-induced ARDS. Meng et al found improved survival in patients treated with these agents (65), though larger trials are needed for confirmation. Bronchodilators (e.g., albuterol) have been used to relieve bronchospasm and reduce inflammation, with studies demonstrating improved lung mechanics but limited data on long-term outcomes. Surfactant replacement therapy, which supplements deficient endogenous surfactant, has shown contradictory results in different studies, necessitating further investigation (14,66).
Anti-Inflammatory Strategies
Corticosteroids and immunomodulatory drugs are utilized to modulate the inflammatory response in sepsis-induced ARDS. A meta-analysis revealed improved survival with corticosteroids, though evidence quality was low (67,68). Drugs targeting cytokines such as IL-6 (e.g., tocilizumab) and IL-10 have shown promise, but their long-term safety and efficacy remain under investigation (69,70).
Vasoactive Agents
NO donors and prostacyclin analogs have been explored for improving vascular function in sepsis-induced ARDS, though evidence on their efficacy is limited (71). In addition, endothelin receptor antagonists (e.g., bosentan) have shown benefits in pulmonary hypertension but require further study in ARDS (72,73).
Statins and Antioxidants
Statins, known for their anti-inflammatory properties, have demonstrated contradictory results in sepsis-related research. Some studies suggested improved outcomes, though evidence quality is low (74-75). Similarly, antioxidants like vitamins C and E have been investigated, but their effects on ARDS outcomes remain inconclusive (76).
Immunonutrition and Extracorporeal Membrane Oxygenation
Immunonutrition, involving nutrient supplementation to support immune function, has shown potential for reducing infections while improving outcomes in critically ill patients, though optimal protocols are unclear (77). ECMO has been used in severe cases of ARDS, with studies reporting benefits in younger patients without significant comorbidities (78).
Proning and Early Mobilization
Proning, or positioning patients on their stomachs, has improved gas exchange and survival in mechanically ventilated ARDS patients. However, its specific efficacy in sepsis-induced ARDS requires further research (79). Early mobilization has been linked to improved functional outcomes and reduced intensive care unit (ICU) stays, though optimal timing and intensity need clarification (80).
Non-Invasive Ventilation
NIV, which avoids intubation, has shown promise in mild-to-moderate ARDS cases, reducing intubation rates while improving survival (81).
Microbiome Analysis in Sepsis-Induced Acute Respiratory Distress Syndrome
The Role of the Microbiome
The human microbiome, comprising trillions of microorganisms, plays a significant role in health and disease. Dysbiosis, or microbial imbalance, has been implicated in sepsis-induced ARDS (82). Alterations in the lung microbiome, including the overgrowth of pathogenic bacteria and reduced beneficial microbes, exacerbate inflammation, increase permeability, and impair lung function. Moreover, gut microbiome changes have been linked to sepsis and ARDS, underscoring the interconnectedness of microbiomes (83,84). In health, the lung microbiome is dominated by Firmicutes and Bacteroidetes, with genera such as Prevotella and Streptococcus being the most prevalent. In disease, inflammation promotes pathogenic species such as Proteobacteria. Microbiome shifts correlate with disease severity, phenotypes, and outcomes, as illustrated in Figure 2 (85). Therefore, understanding these dynamics is key to identifying novel therapeutic targets for sepsis-induced ARDS.
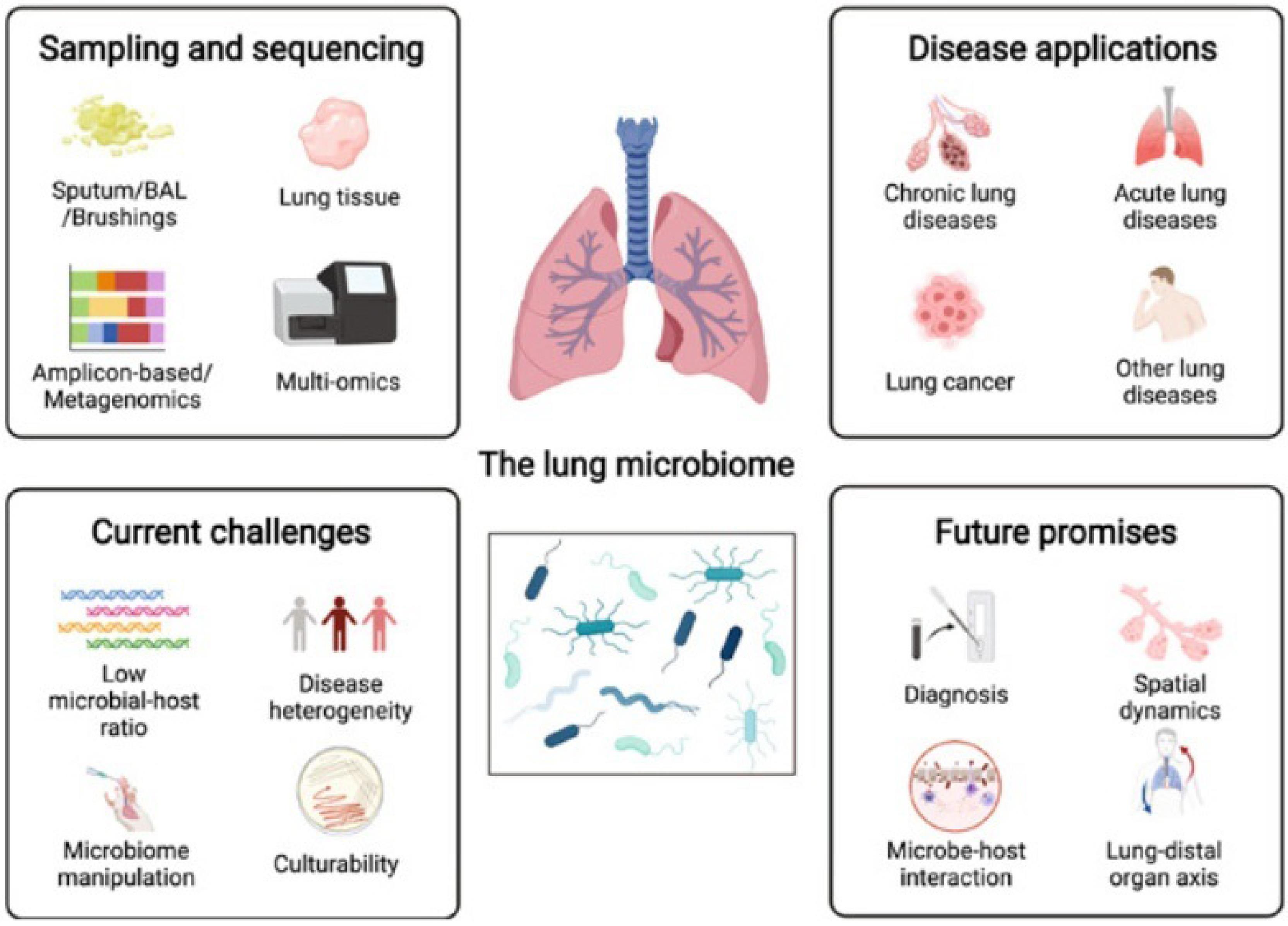
Figure 2.
The Dynamic Lung Microbiome. Reprinted under the terms of the Creative Commons Attribution License (CC BY) (85).
.
The Dynamic Lung Microbiome. Reprinted under the terms of the Creative Commons Attribution License (CC BY) (85).
Strategies for Analyzing the Microbiome
A range of techniques has been developed for investigating the microbiome, among which two are particularly prominent. 16S rRNA gene sequencing targets the variable regions of the 16S rRNA gene, facilitating the detection and quantification of diverse bacterial taxa. In addition, this culture-independent method enables comprehensive profiling of microbial composition and diversity without necessitating the isolation of individual bacterial strains (86). On the other hand, shotgun metagenomics sequences fragmented DNA directly from environmental samples, thereby circumventing the need for prior taxonomic assumptions. This approach not only identifies the constituents of microbial communities but also elucidates their functional genes and potential virulence determinants. Both 16S rRNA gene sequencing and shotgun metagenomics have been pivotal in characterizing microbiome alterations in various pathologies, including sepsis-induced ARDS. Using these methodologies, researchers have delineated distinctive microbial patterns in the pulmonary and gastrointestinal microbiomes that correlate with sepsis-induced ARDS, potentially paving the way for personalized therapeutic strategies tailored to individual microbiomic profiles (87).
Potential Interventions Based on Microbiome Analysis
Targeted modulation of the microbiome presents promising avenues for the therapeutic management of sepsis-induced ARDS. Some of the primary strategies are as follows:
Probiotics and Prebiotics
Probiotics are defined as live microbial supplements that confer health benefits to the host when ingested in sufficient quantities. In contrast, prebiotics are indigestible dietary fibers that selectively foster the proliferation and metabolic activity of beneficial gut bacteria. Both agents have been explored as interventions for sepsis-induced ARDS, demonstrating favorable effects in preclinical animal models and early-phase clinical investigations (88).
Fecal Microbiota Transplantation
FMT entails the introduction of fecal material from healthy donors into the gastrointestinal tract of recipients, aiming to re-establish a balanced microbiota. Its efficacy and safety have been substantiated in conditions such as Clostridioides difficile infection. Further, its utility in sepsis-induced ARDS is under active investigation (89).
Antibiotics and Anti-Virulence Therapy
While broad-spectrum antibiotics remain a mainstay in sepsis management, escalating concerns over multidrug resistance necessitate alternative approaches. In this regard, anti-virulence therapies, which inhibit pathogenic mechanisms without exerting selective pressure for bacterial survival, offer a promising adjunct or alternative to conventional antibiotics (90).
Antimicrobial Stewardship
Effective management of sepsis-induced ARDS critically depends on the judicious application of antimicrobials, encompassing appropriate selection, dosing, and duration. Antimicrobial stewardship programs are essential for minimizing the emergence of resistant organisms and mitigating adverse effects (91). In this context, addressing antibiotic resistance requires a multifaceted approach that spans early diagnosis, evidence-based regimen selection, optimized pharmacokinetics, and vigilant monitoring for complications. Combination therapies, immunomodulation, stringent infection control, and public health education are integral components in this respect (92). Sustained efforts in research, surveillance, protocol refinement, and multidisciplinary collaboration are necessary to entrench a culture of stewardship, thereby improving clinical outcomes, preserving antibiotic efficacy, and fostering responsible use on a systemic level (93).
The lung microbiome significantly influences local and systemic inflammatory responses in pulmonary disorders, such as ARDS. Notably, ARDS is characterized by the pulmonary enrichment of gut-derived bacteria, which serve as salient biomarkers. In critically ill patients, the disruption of the lung microbiome can amplify inflammatory cascades, thereby worsening prognoses. The migration of gut microbes to the pulmonary environment is increasingly recognized as a pathogenic mechanism in sepsis and ARDS, although the precise contribution of gut microflora to lung pathology remains incompletely understood (94). Early microbiome perturbations, including increased bacterial burden, overrepresentation of gastrointestinal taxa, and decreased microbial diversity, are associated with heightened ARDS susceptibility and prolonged dependence on mechanical ventilation. Baseline dysbiosis, potentially induced by environmental exposures (e.g., smoking), may also predispose to post-traumatic ARDS. Viral reactivation, particularly of the herpesviridae family, is frequently observed, reflecting complex, multifactorial drivers of microbial dynamics. Remarkably, ventilator-associated pneumonia is often characterized by the overgrowth of existing bacterial genera rather than the acquisition of new pathogens. While antibiotics target dominant organisms, they may concurrently exacerbate dysbiosis. Studies consistently reveal that the ARDS lung microbiome contains lower gastrointestinal tract bacteria, with their abundance correlating with disease severity (95). Figure 3 displays the mechanisms of lung microbiome disruption in ARDS.
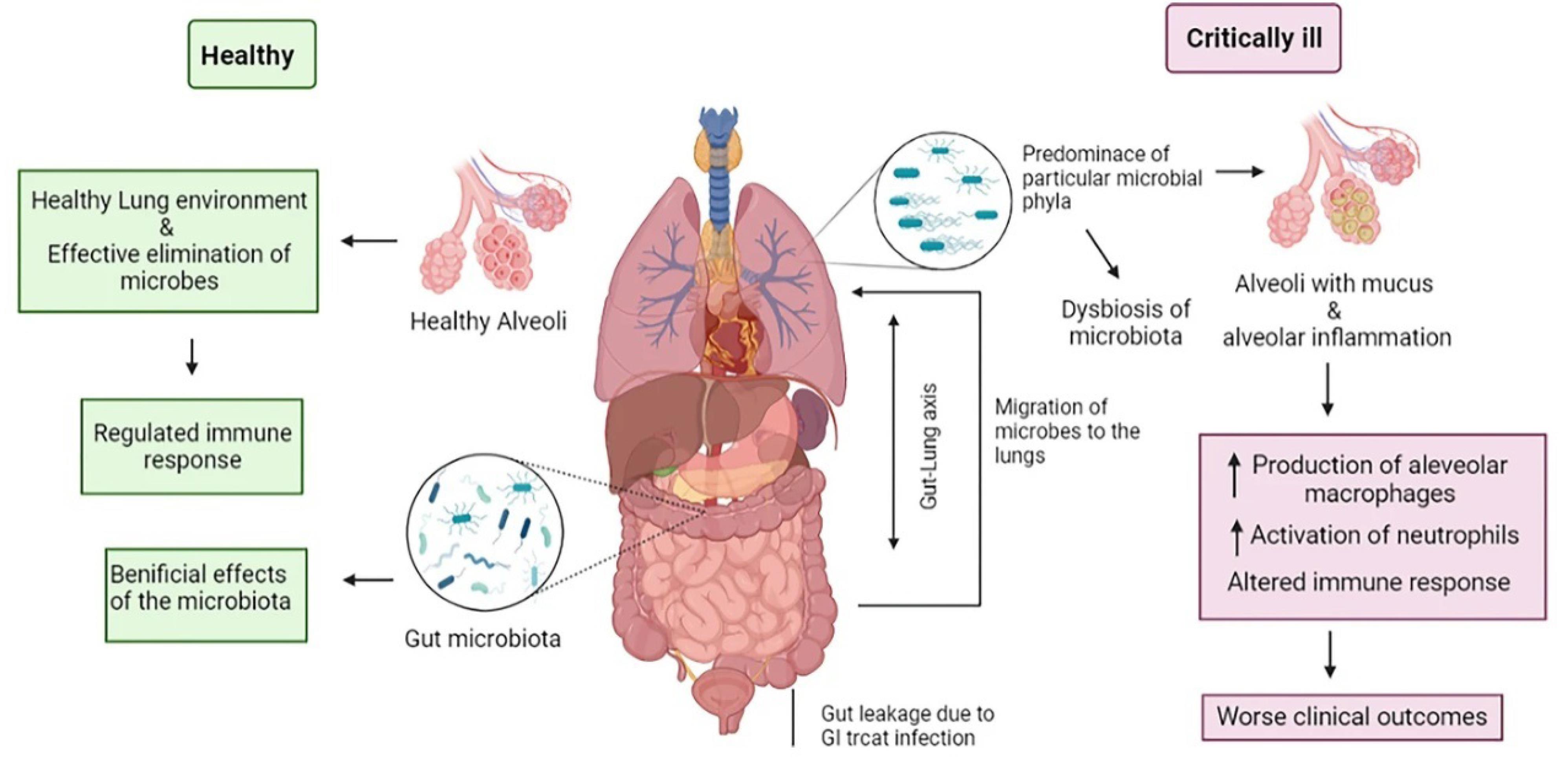
Figure 3.
Mechanisms of Lung Microbiome Disruption in Acute Respiratory Distress Syndrome. Source. (95).
.
Mechanisms of Lung Microbiome Disruption in Acute Respiratory Distress Syndrome. Source. (95).
Nanoparticle-Based Drug Delivery
Advantages of Nanoparticle-Based Drug Delivery
NP-mediated drug delivery systems offer several distinct advantages (e.g., enhanced pharmacokinetic profiles, improved bioavailability, and attenuated systemic toxicity) over traditional modalities (96). These nanoscale vehicles can be precisely engineered to achieve targeted delivery to specific cellular or tissue sites, thereby maximizing therapeutic efficacy while minimizing off-target effects (97). Additionally, NPs can be formulated for controlled and sustained drug release, contributing to increased drug stability, extended half-life, and reduced dosing frequency (98).
Challenges and Limitations
Despite their promise, the clinical translation of NP-based drug delivery faces significant obstacles. Accordingly, achieving efficient and selective NP localization at the intended biological target remains challenging, particularly within the complex and heterogeneous architecture of lung tissue (66). Furthermore, the inherent physicochemical properties of certain NPs may elicit toxicological responses, including inflammation and cellular injury (99). Regulatory pathways for NP therapeutics are still evolving, thereby presenting additional barriers to widespread clinical adoption.
Applications in Sepsis-Induced Acute Respiratory Distress Syndrome
Sepsis-induced ARDS represents a critical condition with persistently high mortality despite advances in supportive care, underscoring the need for innovative therapeutic strategies. NP-based drug delivery holds substantial potential to enhance pulmonary drug targeting while reducing adverse effects. For instance, liposomal formulations have demonstrated improved pulmonary delivery in sepsis-induced ARDS cases. Moreover, NPs can be designed for the co-delivery of multiple pharmacological agents, potentially addressing the complex pathophysiology of sepsis through multifaceted mechanisms. Nonetheless, comprehensive research is required to establish the safety and efficacy profiles of these systems in clinical settings (100).
Optimization of Mechanical Ventilation in Sepsis-Induced Acute Respiratory Distress Syndrome
Protective ventilation protocols, incorporating low tidal volumes and tailored PEEP, are pivotal in minimizing ventilator-induced lung injury in ARDS patients. However, these strategies must be meticulously adapted for burn victims in order to prevent hypoventilation. The presence of inhalational injury exacerbates respiratory compromise via inflammatory responses, edema, and airway obstruction. Adjunctive supportive measures encompass bronchial hygiene, antimicrobial therapy for superimposed infections, and advanced rescue modalities for refractory hypoxemia. Ultimately, ARDS management in the context of burns necessitates a highly individualized strategy that accommodates the unique physiological and pulmonary pathophysiology of each patient (101).
Advanced Modes of Ventilation
Technologies such as adaptive support ventilation utilize the real-time assessments of lung mechanics and gas exchange to dynamically adjust ventilatory support, thereby optimizing oxygen delivery while reducing the risk of ventilator-associated injury. NIVoffers respiratory assistance through external interfaces, obviating the risks associated with invasive airway management (102).
Strategies for Optimizing Mechanical Ventilation
Customizing PEEP and tidal volume settings according to lung-specific parameters allows for personalized mechanical ventilation, thereby enhancing oxygenation while minimizing the risk of barotrauma. The open lung approach employs alveolar recruitment maneuvers followed by adequate PEEP and low tidal volumes, ensuring sustained alveolar patency and minimizing the cyclical injury associated with repetitive collapse and re-expansion (103).
Open Lung Approach
To address atelectasis and optimize gas exchange in sepsis-induced respiratory failure, recruitment maneuvers transiently apply elevated pressures or tidal volumes to reinflate collapsed alveoli. High-frequency oscillatory ventilation achieves gas exchange via rapid oscillations, thereby enabling lower tidal volumes and reduced risk of ventilator-induced injury. These advanced ventilation modalities, in conjunction with the meticulous application of lung-protective strategies and open lung approaches, empower clinicians to effectively manage respiratory compromise in sepsis, thereby reducing morbidity and mortality (104).
Big Data Analytics in Sepsis-Induced Acute Respiratory Distress Syndrome
Integration of Data From Various Sources
The convergence of data from EHRs, clinical trials, and omics platforms has opened new frontiers in managing sepsis-induced ARDS. EHRs provide comprehensive patient profiles, encompassing demographic, comorbid, physiological, and laboratory data, which inform tailored management strategies (105). Clinical trials contribute critical insights into the efficacy and safety of emerging interventions, while omics technologies elucidate the molecular architecture and biomarker signatures underlying ARDS. Thus, integrating these heterogeneous datasets through sophisticated analytics and AI has the potential to revolutionize sepsis care (106).
Potential Insights and Benefits
Utilizing big data analytics enables the implementation of precision medicine in sepsis-induced ARDS, with interventions customized to individual patient risk factors and genetic backgrounds. Predictive modeling can anticipate disease progression, facilitating earlier intervention and more informed clinical decision-making. Moreover, stratifying patients by risk allows for targeted preventive measures, ultimately reducing the incidence of ARDS, improving outcomes, and diminishing long-term healthcare impacts (20).
Challenges and Limitations
Realizing the transformative potential of big data analytics in sepsis-induced ARDS hinges on overcoming challenges related to data integrity, security, accessibility, and ethical stewardship. Ensuring algorithmic transparency and interpretability is vital for timely and actionable clinical insights. Human oversight remains essential to complement ML, fostering confidence and collaboration. The standardization of data sources, equitable access to analytics tools, and ongoing adaptation to new discoveries are crucial in this regard. It should be noted that success requires a holistic approach that balances data sharing with privacy, inclusivity, and responsible innovation, enabling equitable transformation of sepsis-induced ARDS management on a global scale (107).
Virtual Reality Rehabilitation
Benefits of Virtual Reality Rehabilitation
VR-based rehabilitation offers patients the opportunity to commence mobilization and physical therapy earlier than is often feasible with traditional modalities, potentially expediting recovery and enhancing clinical outcomes. VR provides a highly controlled and interactive environment, reducing the risk of rehabilitation-related complications, such as falls or secondary injuries. Furthermore, this immersive approach allows patients to safely and repetitively practice targeted movements and exercises, promoting functional improvement (108).
Challenges and Limitations
The widespread adoption of VR rehabilitation is impeded by the significant costs associated with acquiring and maintaining the necessary technology and software, which may be prohibitive for many healthcare institutions. Accessibility issues are further compounded in rural or underserved regions. Additionally, patient acceptance can present a barrier, as unfamiliarity with VR or skepticism regarding its effectiveness may deter participation. Sustaining patient motivation and adherence to VR-based protocols represents an additional challenge for clinical teams (109). Accordingly, an informed understanding of these benefits and limitations is essential for healthcare providers seeking to incorporate VR into rehabilitation programs and optimize patient outcomes.
Personalized Medicine in Sepsis-Induced Acute Respiratory Distress Syndrome
Precision medicine approaches offer transformative possibilities for the individualized management of sepsis-induced ARDS by enabling care that is holistically tailored to each patient’s unique clinical, genetic, and environmental context. Incorporating natural and traditional remedies that resonate with a patient’s cultural values (e.g., herbal therapies, acupuncture, or meditation) may complement conventional anti-inflammatory and regenerative treatments (110). This integrative paradigm addresses the patient as a whole and fosters enhanced engagement and satisfaction with care. Leveraging detailed genomic, lifestyle, and environmental data further refines therapy selection, thereby allowing clinicians to anticipate and mitigate risks, such as those related to genetic predisposition or prior smoking history (66). It is noteworthy that identifying individuals at high risk for sepsis or ARDS through genetic screening enables proactive surveillance and early intervention strategies, potentially forestalling disease onset. In general, personalized medicine in this domain aims to deliver truly individualized, comprehensive care by aligning therapeutic interventions with the distinct risk profiles and needs of each patient, thereby improving prevention, outcomes, and the overall healthcare burden (111).
Artificial Intelligence and Machine Learning
AI and ML have emerged as transformative technologies in critical care, especially regarding the diagnosis and management of sepsis-induced ARDS. This literature review explored the burgeoning role of AI and ML in this context. Recent advances in these fields have introduced new opportunities to enhance the management of sepsis-induced ARDS (112). Figure 4 illustrates two deployment models of the COMPOSER platform. In the evaluation phase (panel b), test data pass through a weighted input layer and an encoder to produce a new representation H (2). Conformal prediction evaluates whether H (2) matches the conformity standards established by the training set; the sample proceeds to the sepsis risk predictor if conformity is confirmed at a specified confidence level ε. In contrast, panel (c) demonstrates model deployment without conformal prediction, omitting this safeguard (113).
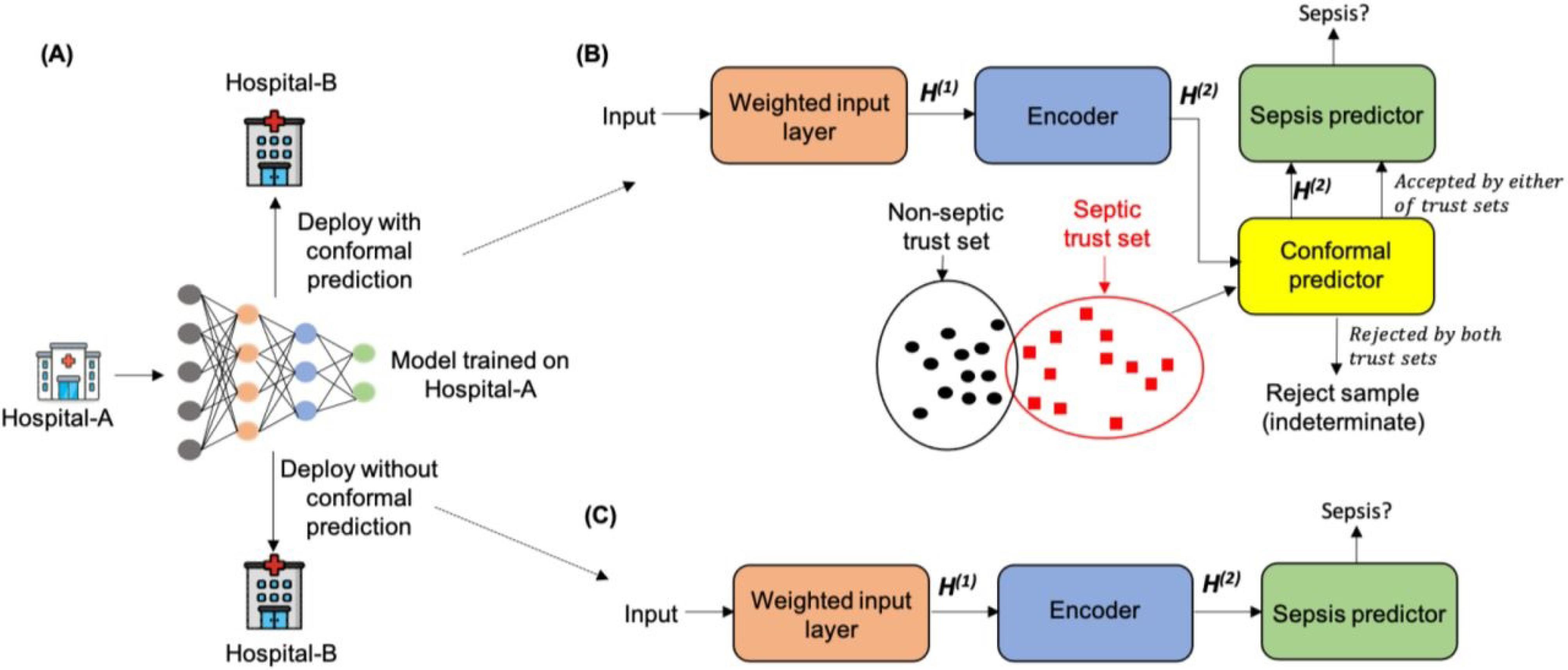
Figure 4.
The Role of Artificial Intelligence and Machine Learning in Managing Sepsis-Induced Acute respiratory distress syndrome. Reprinted under the terms of the Creative Commons Attribution License (CC BY) (113).
.
The Role of Artificial Intelligence and Machine Learning in Managing Sepsis-Induced Acute respiratory distress syndrome. Reprinted under the terms of the Creative Commons Attribution License (CC BY) (113).
Predictive Modeling
Predictive modeling with AI and ML algorithms is poised to revolutionize medicine, especially in intensive care. These models can discern patterns and relationships beyond human capability by synthesizing vast datasets, encompassing EHRs, imaging, and laboratory findings. In addition, AI-driven analysis provides prognostic insights regarding survival, recovery likelihood, and ICU admission requirements (16). This information empowers clinicians to optimize triage, allocate resources effectively, and tailor treatment plans. Further, modeling the trajectory of sepsis-induced ARDS enables early identification of clinical deterioration or improvement, supporting timely and individualized intervention (19).
Clinical Decision Support Systems
AI-enhanced CDSSs offer real-time, evidence-based recommendations for diagnosis, therapy, and monitoring by integrating patient-specific data with current medical knowledge. Furthermore, these systems can suggest diagnostic and therapeutic options adapted to each patient’s needs, thereby reducing cognitive errors, improving operational efficiency, and streamlining clinical workflows. Moreover, continuous monitoring of vital signs and laboratory data enables prompt alerts for deviations or clinical deterioration, facilitating timely intervention and improved patient safety (114).
Natural Language Processing
NLP represents another frontier for AI and ML in healthcare, enabling the extraction of actionable insights from unstructured data sources (e.g., clinical notes and radiology reports). Additionally, NLP-powered chatbots can mediate communication among patients, families, and clinicians, addressing concerns and symptoms in real time, thereby enhancing engagement and satisfaction (115). By analyzing large corpora of clinical text, NLP can also uncover trends and patterns that inform quality improvement, risk stratification, and research. The integration of AI and ML into sepsis-induced ARDS management holds the potential to transform patient care, improve outcomes, and reduce costs, although challenges remain in their implementation and validation (116).
Conclusion
The integration of omics technologies, advanced imaging modalities, and biomarker discovery has yielded significant advances in understanding the complex pathophysiology of sepsis-induced ARDS, facilitating more accurate diagnosis and enabling the development of personalized treatment strategies. Emerging therapies, including lung-targeted interventions, anti-inflammatory agents, and microbiome modulation, demonstrate potential for improving clinical outcomes. Further enhancements have been achieved through optimized ventilation protocols and the application of big data analytics, AI, and ML, all contributing to superior clinical decision-making. Nonetheless, key challenges persist, such as the need for larger-scale validation of new therapies, translation of biomarker findings to clinical practice, and the management of risks associated with NP-based delivery. In addition, the high costs and limited accessibility of some advanced technologies impede their widespread use, particularly in resource-constrained environments.
Recommendations
Several strategic recommendations are proposed to overcome current barriers and further progress in the management of sepsis-induced ARDS. First, there is an urgent need for robust, multicenter randomized controlled trials to establish the safety and efficacy of novel therapies across diverse populations. Second, efforts should be intensified to standardize and expedite the clinical translation of biomarker discoveries. Third, additional research is warranted to refine NP-based drug delivery systems, thereby enhancing their safety and specificity. Fourth, prioritizing the development of affordable and user-friendly advanced technologies will increase their adoption in varied healthcare contexts. Fifth, interdisciplinary collaboration should be promoted to integrate insights from omics, imaging, and clinical datasets, thus fostering the creation of comprehensive predictive models and individualized therapeutic plans. Finally, as AI and ML become more prevalent in clinical care, ethical considerations and the protection of patient privacy must remain paramount.
Acknowledgments
The author thanks all the researchers who have made great efforts in their studies. Moreover, he is grateful to the editors, reviewers, and readers of this journal for their valuable contributions and support.
Competing Interests
The author declares that he has no competing interests.
Ethical Approval
Not applicable.
Funding
The corresponding author supplied all study materials. He received no financial support for this study.
References
- Liu L, Wu L, Chen Y, Deng R, Hu Y, Tu Y. Clinical management of sepsis-associated acute respiratory distress syndrome: current evidence and future directions. Front Med (Lausanne) 2025; 12:1531275. doi: 10.3389/fmed.2025.1531275 [Crossref] [ Google Scholar]
- Garduno A, Cusack R, Leone M, Einav S, Martin-Loeches I. Multi-omics endotypes in ICU sepsis-induced immunosuppression. Microorganisms 2023; 11(5):1119. doi: 10.3390/microorganisms11051119 [Crossref] [ Google Scholar]
- Chang Y, Yoo HJ, Kim SJ, Lee K, Lim CM, Hong SB. A targeted metabolomics approach for sepsis-induced ARDS and its subphenotypes. Crit Care 2023; 27(1):263. doi: 10.1186/s13054-023-04552-0 [Crossref] [ Google Scholar]
- Tullo G, Candelli M, Gasparrini I, Micci S, Franceschi F. Ultrasound in sepsis and septic shock-from diagnosis to treatment. J Clin Med 2023; 12(3):1185. doi: 10.3390/jcm12031185 [Crossref] [ Google Scholar]
- Gozzi L, Cozzi D, Cavigli E, Moroni C, Giannessi C, Zantonelli G. Primary lymphoproliferative lung diseases: imaging and multidisciplinary approach. Diagnostics (Basel) 2023; 13(7):1360. doi: 10.3390/diagnostics13071360 [Crossref] [ Google Scholar]
- McCague C, Ramlee S, Reinius M, Selby I, Hulse D, Piyatissa P. Introduction to radiomics for a clinical audience. Clin Radiol 2023; 78(2):83-98. doi: 10.1016/j.crad.2022.08.149 [Crossref] [ Google Scholar]
- Arora J, Mendelson AA, Fox-Robichaud A. Sepsis: network pathophysiology and implications for early diagnosis. Am J Physiol Regul Integr Comp Physiol 2023; 324(5):R613-24. doi: 10.1152/ajpregu.00003.2023 [Crossref] [ Google Scholar]
- Li Q, Zheng H, Chen B. Identification of macrophage-related genes in sepsis-induced ARDS using bioinformatics and machine learning. Sci Rep 2023; 13(1):9876. doi: 10.1038/s41598-023-37162-5 [Crossref] [ Google Scholar]
- Liu S-Y, Ruan H, Li S-s. HIF-1α: a bridge connecting sepsis and acute respiratory distress syndrome. European Journal of Medical Research 2025; 30(1):827. doi: 10.1186/s40001-025-03107-z [Crossref] [ Google Scholar]
- Kuperminc E, Heming N, Carlos M, Annane D. Corticosteroids in ARDS. J Clin Med 2023;12(9). doi: 10.3390/jcm12093340.
- Marascio N, Scarlata GG, Romeo F, Cicino C, Trecarichi EM, Quirino A. The role of gut microbiota in the clinical outcome of septic patients: state of the art and future perspectives. Int J Mol Sci 2023; 24(11):9307. doi: 10.3390/ijms24119307 [Crossref] [ Google Scholar]
- Cheng X, Xie Q, Sun Y. Advances in nanomaterial-based targeted drug delivery systems. Front Bioeng Biotechnol 2023; 11:1177151. doi: 10.3389/fbioe.2023.1177151 [Crossref] [ Google Scholar]
- Hennessey E, Bittner E, White P, Kovar A, Meuchel L. Intraoperative ventilator management of the critically ill patient. Anesthesiol Clin 2023; 41(1):121-40. doi: 10.1016/j.anclin.2022.11.004 [Crossref] [ Google Scholar]
- Fujishima S. Guideline-based management of acute respiratory failure and acute respiratory distress syndrome. J Intensive Care 2023; 11(1):10. doi: 10.1186/s40560-023-00658-3 [Crossref] [ Google Scholar]
- Wang Q, Liu Y, Fu Y, Liu C, Li J, Dang H. Analysis of predictors of mortality and clinical outcomes of different subphenotypes for moderate-to-severe pediatric acute respiratory distress syndrome: a prospective single-center study. Front Pediatr 2022; 10:1019314. doi: 10.3389/fped.2022.1019314 [Crossref] [ Google Scholar]
- Bai Y, Xia J, Huang X, Chen S, Zhan Q. Using machine learning for the early prediction of sepsis-associated ARDS in the ICU and identification of clinical phenotypes with differential responses to treatment. Front Physiol 2022; 13:1050849. doi: 10.3389/fphys.2022.1050849 [Crossref] [ Google Scholar]
- Velez M, Lugo-Agudelo LH, Patiño Lugo DF, Glenton C, Posada AM, Mesa Franco LF. Factors that influence the provision of home-based rehabilitation services for people needing rehabilitation: a qualitative evidence synthesis. Cochrane Database Syst Rev 2023; 2(2):CD014823. doi: 10.1002/14651858.Cd014823 [Crossref] [ Google Scholar]
- Battaglini D, Al-Husinat L, Normando AG, Leme AP, Franchini K, Morales M. Personalized medicine using omics approaches in acute respiratory distress syndrome to identify biological phenotypes. Respir Res 2022; 23(1):318. doi: 10.1186/s12931-022-02233-0 [Crossref] [ Google Scholar]
- Pai KC, Chao WC, Huang YL, Sheu RK, Chen LC, Wang MS. Artificial intelligence-aided diagnosis model for acute respiratory distress syndrome combining clinical data and chest radiographs. Digit Health 2022; 8:20552076221120317. doi: 10.1177/20552076221120317 [Crossref] [ Google Scholar]
- Okada Y, Mertens M, Liu N, Lam SS, Ong ME. AI and machine learning in resuscitation: ongoing research, new concepts, and key challenges. Resusc Plus 2023; 15:100435. doi: 10.1016/j.resplu.2023.100435 [Crossref] [ Google Scholar]
- Sun M, Yang Q, Hu C, Zhang H, Xing L. Identification and validation of autophagy-related genes in sepsis-induced acute respiratory distress syndrome and immune infiltration. J Inflamm Res 2022; 15:2199-212. doi: 10.2147/jir.S355225 [Crossref] [ Google Scholar]
- Daniel M, Bedoui Y, Vagner D, Raffray L, Ah-Pine F, Doray B. Pathophysiology of sepsis and genesis of septic shock: the critical role of mesenchymal stem cells (MSCs). Int J Mol Sci 2022; 23(16):9274. doi: 10.3390/ijms23169274 [Crossref] [ Google Scholar]
- Cusack R, Bos LD, Povoa P, Martin-Loeches I. Endothelial dysfunction triggers acute respiratory distress syndrome in patients with sepsis: a narrative review. Front Med (Lausanne) 2023; 10:1203827. doi: 10.3389/fmed.2023.1203827 [Crossref] [ Google Scholar]
- Gong H, Chen Y, Chen M, Li J, Zhang H, Yan S. Advanced development and mechanism of sepsis-related acute respiratory distress syndrome. Front Med (Lausanne) 2022; 9:1043859. doi: 10.3389/fmed.2022.1043859 [Crossref] [ Google Scholar]
- Liu D, Huang SY, Sun JH, Zhang HC, Cai QL, Gao C. Sepsis-induced immunosuppression: mechanisms, diagnosis and current treatment options. Mil Med Res 2022; 9(1):56. doi: 10.1186/s40779-022-00422-y [Crossref] [ Google Scholar]
- Wu J, Lan Y, Wu J, Zhu K. Sepsis-induced acute lung injury is alleviated by small molecules from dietary plants via pyroptosis modulation. J Agric Food Chem 2023; 71(32):12153-66. doi: 10.1021/acs.jafc.2c08926 [Crossref] [ Google Scholar]
- Bos LD, Ware LB. Acute respiratory distress syndrome: causes, pathophysiology, and phenotypes. Lancet 2022; 400(10358):1145-56. doi: 10.1016/s0140-6736(22)01485-4 [Crossref] [ Google Scholar]
- Geyer-Roberts E, Lacatusu DA, Kester J, Foster-Moumoutjis G, Sidiqi M. Preventative management of sepsis-induced acute respiratory distress syndrome in the geriatric population. Cureus 2023; 15(2):e34680. doi: 10.7759/cureus.34680 [Crossref] [ Google Scholar]
- Chiumello D, Modafferi L, Fratti I. Risk factors and mortality in elderly ARDS COVID-19 compared to patients without COVID-19. J Clin Med 2022; 11(17):5180. doi: 10.3390/jcm11175180 [Crossref] [ Google Scholar]
- Prasertsan P, Anantasit N, Walanchapruk S, Roekworachai K, Samransamruajkit R, Vaewpanich J. Sepsis-related pediatric acute respiratory distress syndrome: a multicenter prospective cohort study. Turk J Emerg Med 2023; 23(2):96-103. doi: 10.4103/tjem.tjem_237_22 [Crossref] [ Google Scholar]
- Batra R, Whalen W, Alvarez-Mulett S, Gomez-Escobar LG, Hoffman KL, Simmons W. Multi-omic comparative analysis of COVID-19 and bacterial sepsis-induced ARDS. PLoS Pathog 2022; 18(9):e1010819. doi: 10.1371/journal.ppat.1010819 [Crossref] [ Google Scholar]
- Feng J, Pang J, He D, Wu Z, Li Q, Ji P. Identification of genes with altered methylation and its role in early diagnosis of sepsis-induced acute respiratory distress syndrome. Int J Gen Med 2021; 14:243-53. doi: 10.2147/ijgm.S287960 [Crossref] [ Google Scholar]
- Suarez-Pajes E, Tosco-Herrera E, Ramirez-Falcon M, Gonzalez-Barbuzano S, Hernandez-Beeftink T, Guillen-Guio B. Genetic determinants of the acute respiratory distress syndrome. J Clin Med 2023; 12(11):3713. doi: 10.3390/jcm12113713 [Crossref] [ Google Scholar]
- Palma Medina LM, Babačić H, Dzidic M, Parke Å, Garcia M, Maleki KT. Targeted plasma proteomics reveals signatures discriminating COVID-19 from sepsis with pneumonia. Respir Res 2023; 24(1):62. doi: 10.1186/s12931-023-02364-y [Crossref] [ Google Scholar]
- Gong R, Luo H, Long G, Xu J, Huang C, Zhou X. Integrative proteomic profiling of lung tissues and blood in acute respiratory distress syndrome. Front Immunol 2023; 14:1158951. doi: 10.3389/fimmu.2023.1158951 [Crossref] [ Google Scholar]
- Batra R, Uni R, Akchurin OM, Alvarez-Mulett S, Gómez-Escobar LG, Patino E. Urine-based multi-omic comparative analysis of COVID-19 and bacterial sepsis-induced ARDS. Mol Med 2023; 29(1):13. doi: 10.1186/s10020-023-00609-6 [Crossref] [ Google Scholar]
- Yang B, Gao Z, Li QS, Zhang XY, Song L, Wang YN. Proteomic analysis and identification reveal the anti-inflammatory mechanism of clofazimine on lipopolysaccharide-induced acute lung injury in mice. Inflamm Res 2022; 71(10-11):1327-45. doi: 10.1007/s00011-022-01623-w [Crossref] [ Google Scholar]
- Juanes-Velasco P, García-Vaquero ML, Landeira-Viñuela A, Lopez-Campos JL, Marín C, Lecrevisse Q. Systematic evaluation of plasma signaling cascades by functional proteomics approaches: SARS-CoV-2 infection as model. Proteomics Clin Appl 2022; 16(6):e2100100. doi: 10.1002/prca.202100100 [Crossref] [ Google Scholar]
- Bruzzone C, Conde R, Embade N, Mato JM, Millet O. Metabolomics as a powerful tool for diagnostic, pronostic and drug intervention analysis in COVID-19. Front Mol Biosci 2023; 10:1111482. doi: 10.3389/fmolb.2023.1111482 [Crossref] [ Google Scholar]
- McClintock CR, Mulholland N, Krasnodembskaya AD. Biomarkers of mitochondrial dysfunction in acute respiratory distress syndrome: a systematic review and meta-analysis. Front Med (Lausanne) 2022; 9:1011819. doi: 10.3389/fmed.2022.1011819 [Crossref] [ Google Scholar]
- Tian C, Wang K, Zhao M, Cong S, Di X, Li R. Extracellular vesicles participate in the pathogenesis of sepsis. Front Cell Infect Microbiol 2022; 12:1018692. doi: 10.3389/fcimb.2022.1018692 [Crossref] [ Google Scholar]
- Ning L, Shishi Z, Bo W, Huiqing L. Targeting immunometabolism against acute lung injury. Clin Immunol 2023; 249:109289. doi: 10.1016/j.clim.2023.109289 [Crossref] [ Google Scholar]
- Addissouky T, Ali MM, El Sayed IE, Alubiady MH. Realizing the promise of artificial intelligence in hepatocellular carcinoma through opportunities and recommendations for responsible translation. J Online Inform 2024; 9(1):70-9. doi: 10.15575/join.v9i1.1297 [Crossref] [ Google Scholar]
- Addissouky TA, Ali MM, El Sayed IE, Wang Y, El Baz A, Elarabany N. Preclinical promise and clinical challenges for innovative therapies targeting liver fibrogenesis. Arch Gastroenterol Res 2023; 4(1):14-23. doi: 10.33696/Gastroenterology.4.044 [Crossref] [ Google Scholar]
- Mailem RC, Tayo LL. Drug repurposing using gene co-expression and module preservation analysis in acute respiratory distress syndrome (ARDS), systemic inflammatory response syndrome (SIRS), sepsis, and COVID-19. Biology (Basel) 2022; 11(12):1827. doi: 10.3390/biology11121827 [Crossref] [ Google Scholar]
- Mo J, Yang Y, Feng J, Lei Y, Huang S, Cen W. Single-cell analysis reveals dysregulated inflammatory response in peripheral blood immunity in patients with acute respiratory distress syndrome. Front Cell Dev Biol 2023; 11:1199122. doi: 10.3389/fcell.2023.1199122 [Crossref] [ Google Scholar]
- Vanhorebeek I, Van den Berghe G. The epigenetic legacy of ICU feeding and its consequences. Curr Opin Crit Care 2023; 29(2):114-22. doi: 10.1097/mcc.0000000000001021 [Crossref] [ Google Scholar]
- Albers J, Wagner WL, Fiedler MO, Rothermel A, Wünnemann F, Di Lillo F. High resolution propagation-based lung imaging at clinically relevant X-ray dose levels. Sci Rep 2023; 13(1):4788. doi: 10.1038/s41598-023-30870-y [Crossref] [ Google Scholar]
- Han X, Chen L, Fan Y, Alwalid O, Jia X, Zheng Y. Longitudinal assessment of chest CT findings and pulmonary function after COVID-19 infection. Radiology 2023; 307(2):e222888. doi: 10.1148/radiol.222888 [Crossref] [ Google Scholar]
- Lee CY. Interstitial lung disease-from pulmonary perspective to pathogenesis, multidisciplinary approach and treatment. Int J Rheum Dis 2023; 26(5):823-4. doi: 10.1111/1756-185x.14626 [Crossref] [ Google Scholar]
- Osawa EA, Kleiman JF, Maciel AT. Acute respiratory distress syndrome following administration of gadolinium contrast agent: a case report. J Med Case Rep 2022; 16(1):421. doi: 10.1186/s13256-022-03643-w [Crossref] [ Google Scholar]
- Ge C, Deng F, Chen W, Ye Z, Zhang L, Ai Y. Machine learning for early prediction of sepsis-associated acute brain injury. Front Med (Lausanne) 2022; 9:962027. doi: 10.3389/fmed.2022.962027 [Crossref] [ Google Scholar]
- Martinez-Orengo N, Tahmazian S, Lai J, Wang Z, Sinharay S, Schreiber-Stainthorp W. Assessing organ-level immunoreactivity in a rat model of sepsis using TSPO PET imaging. Front Immunol 2022; 13:1010263. doi: 10.3389/fimmu.2022.1010263 [Crossref] [ Google Scholar]
- Addissouky TA, Ali MM, El Sayed IE, Wang Y, Khalil AA. Translational insights into molecular mechanisms of chemical hepatocarcinogenesis for improved human risk assessment. Adv Clin Toxicol 2024; 9(1):294. doi: 10.23880/act-16000294 [Crossref] [ Google Scholar]
- Addissouky TA, Ali MM, El Sayed IE, Wang Y. Emerging advanced approaches for diagnosis and inhibition of liver fibrogenesis. Egypt J Intern Med 2024; 36(1):19. doi: 10.1186/s43162-024-00283-y [Crossref] [ Google Scholar]
- Zeng C, Zhu M, Motta-Ribeiro G, Lagier D, Hinoshita T, Zang M. Dynamic lung aeration and strain with positive end-expiratory pressure individualized to maximal compliance versus ARDSNet low-stretch strategy: a study in a surfactant depletion model of lung injury. Crit Care 2023; 27(1):307. doi: 10.1186/s13054-023-04591-7 [Crossref] [ Google Scholar]
- Zhu Q, Barnes CE, Mannes PZ, Latoche JD, Day KE, Nedrow JR. Targeted imaging of very late antigen-4 for noninvasive assessment of lung inflammation-fibrosis axis. EJNMMI Res 2023; 13(1):55. doi: 10.1186/s13550-023-01006-0 [Crossref] [ Google Scholar]
- Alimohammadi M, Mohammad RN, Rahimi A, Faramarzi F, Alizadeh-Navaei R, Rafiei A. The effect of immunomodulatory properties of naringenin on the inhibition of inflammation and oxidative stress in autoimmune disease models: a systematic review and meta-analysis of preclinical evidence. Inflamm Res 2022; 71(10-11):1127-42. doi: 10.1007/s00011-022-01599-7 [Crossref] [ Google Scholar]
- Zhang S, Chen YC, Riezk A, Ming D, Tsvik L, Sützl L. Rapid measurement of lactate in the exhaled breath condensate: biosensor optimization and in-human proof of concept. ACS Sens 2022; 7(12):3809-16. doi: 10.1021/acssensors.2c01739 [Crossref] [ Google Scholar]
- Grasselli G, Calfee CS, Camporota L, Poole D, Amato MB, Antonelli M. ESICM guidelines on acute respiratory distress syndrome: definition, phenotyping and respiratory support strategies. Intensive Care Med 2023; 49(7):727-59. doi: 10.1007/s00134-023-07050-7 [Crossref] [ Google Scholar]
- Marshall JC, Leligdowicz A. Gaps and opportunities in sepsis translational research. EBioMedicine 2022; 86:104387. doi: 10.1016/j.ebiom.2022.104387 [Crossref] [ Google Scholar]
- von Groote T, Meersch-Dini M. Biomarkers for the prediction and judgement of sepsis and sepsis complications: a step towards precision medicine?. J Clin Med 2022; 11(19):5782. doi: 10.3390/jcm11195782 [Crossref] [ Google Scholar]
- Addissouky TA, El Sayed IE, Ali MM, Wang Y, El Baz A, Khalil AA. Latest advances in hepatocellular carcinoma management and prevention through advanced technologies. Egypt Liver J 2024; 14(1):2. doi: 10.1186/s43066-023-00306-3 [Crossref] [ Google Scholar]
- Addissouky TA, Ali MM, El Sayed IE, Wang Y. Transforming screening, risk stratification, and treatment optimization in chronic liver disease through data science and translational innovation. Indones J Gastroenterol Hepatol Dig Endosc 2024; 25(1):53-62. doi: 10.24871/251202453-62 [Crossref] [ Google Scholar]
- Meng L, Liao X, Wang Y, Chen L, Gao W, Wang M. Pharmacologic therapies of ARDS: from natural herb to nanomedicine. Front Pharmacol 2022; 13:930593. doi: 10.3389/fphar.2022.930593 [Crossref] [ Google Scholar]
- Winkler MS, Osuchowski MF, Payen D, Torres A, Dickel S, Skirecki T. Renaissance of glucocorticoids in critical care in the era of COVID-19: ten urging questions. Crit Care 2022; 26(1):308. doi: 10.1186/s13054-022-04185-9 [Crossref] [ Google Scholar]
- Ilias I, Vassiliou AG, Keskinidou C, Vrettou CS, Orfanos S, Kotanidou A. Changes in cortisol secretion and corticosteroid receptors in COVID-19 and non COVID-19 critically ill patients with sepsis/septic shock and scope for treatment. Biomedicines 2023; 11(7):1801. doi: 10.3390/biomedicines11071801 [Crossref] [ Google Scholar]
- Al-Sofyani KA. Corticosteroids treatment for pediatric acute respiratory syndrome: a critical review. Saudi Med J 2023; 44(5):440-9. doi: 10.15537/smj.2023.44.5.20220672 [Crossref] [ Google Scholar]
- Carlini V, Noonan DM, Abdalalem E, Goletti D, Sansone C, Calabrone L. The multifaceted nature of IL-10: regulation, role in immunological homeostasis and its relevance to cancer, COVID-19 and post-COVID conditions. Front Immunol 2023; 14:1161067. doi: 10.3389/fimmu.2023.1161067 [Crossref] [ Google Scholar]
- Korkmaz FT, Traber KE. Innate immune responses in pneumonia. Pneumonia (Nathan) 2023; 15(1):4. doi: 10.1186/s41479-023-00106-8 [Crossref] [ Google Scholar]
- Janssen M, Endeman H, Bos LDJ. Targeted immunomodulation: a primer for intensivists. Intensive Care Med 2023; 49(4):462-4. doi: 10.1007/s00134-023-07009-8 [Crossref] [ Google Scholar]
- Addissouky TA, El Sayed IE, Ali MM, Wang Y, El Baz A, Khalil AA. Can vaccines stop cancer before it starts? Assessing the promise of prophylactic immunization against high-risk preneoplastic lesions. J Cell Immunol 2023; 5(4):127-40. doi: 10.33696/immunology.5.178 [Crossref] [ Google Scholar]
- Maneta E, Aivalioti E, Tual-Chalot S, Emini Veseli B, Gatsiou A, Stamatelopoulos K. Endothelial dysfunction and immunothrombosis in sepsis. Front Immunol 2023; 14:1144229. doi: 10.3389/fimmu.2023.1144229 [Crossref] [ Google Scholar]
- Pienkos SM, Moore AR, Guan J, Levitt JE, Matthay MA, Baron RM. Effect of total cholesterol and statin therapy on mortality in ARDS patients: a secondary analysis of the SAILS and HARP-2 trials. Crit Care 2023; 27(1):126. doi: 10.1186/s13054-023-04387-9 [Crossref] [ Google Scholar]
- Nesson ET, McDowell SA. Innovations in evaluating statin benefit and efficacy in Staphylococcus aureus intracellular infection management. Int J Mol Sci 2022; 23(21):13006. doi: 10.3390/ijms232113006 [Crossref] [ Google Scholar]
- Abelli J, Méndez-Valdés G, Gómez-Hevia F, Bragato MC, Chichiarelli S, Saso L. Potential antioxidant multitherapy against complications occurring in sepsis. Biomedicines 2022; 10(12):3088. doi: 10.3390/biomedicines10123088 [Crossref] [ Google Scholar]
- Velotti F, Costantini L, Merendino N. Omega-3 polyunsaturated fatty acids (n-3 PUFAs) for immunomodulation in COVID-19 related acute respiratory distress syndrome (ARDS). J Clin Med 2022; 12(1):304. doi: 10.3390/jcm12010304 [Crossref] [ Google Scholar]
- Alessandri F, Di Nardo M, Ramanathan K, Brodie D, MacLaren G. Extracorporeal membrane oxygenation for COVID-19-related acute respiratory distress syndrome: a narrative review. J Intensive Care 2023; 11(1):5. doi: 10.1186/s40560-023-00654-7 [Crossref] [ Google Scholar]
- Lai C, Monnet X, Teboul JL. Hemodynamic implications of prone positioning in patients with ARDS. Crit Care 2023; 27(1):98. doi: 10.1186/s13054-023-04369-x [Crossref] [ Google Scholar]
- Watanabe S, Hirasawa J, Naito Y, Mizutani M, Uemura A, Nishimura S. Association between the early mobilization of mechanically ventilated patients and independence in activities of daily living at hospital discharge. Sci Rep 2023; 13(1):4265. doi: 10.1038/s41598-023-31459-1 [Crossref] [ Google Scholar]
- Mina B, Newton A, Hadda V. Noninvasive ventilation in treatment of respiratory failure-related COVID-19 infection: review of the literature. Can Respir J 2022; 2022:9914081. doi: 10.1155/2022/9914081 [Crossref] [ Google Scholar]
- Hu X, Han Z, Zhou R, Su W, Gong L, Yang Z. Altered gut microbiota in the early stage of acute pancreatitis were related to the occurrence of acute respiratory distress syndrome. Front Cell Infect Microbiol 2023; 13:1127369. doi: 10.3389/fcimb.2023.1127369 [Crossref] [ Google Scholar]
- Addissouky TA. Emerging therapeutics targeting cellular stress pathways to mitigate end-organ damage in type 1 diabetes. Avicenna J Med Biochem 2024; 12(1):39-46. doi: 10.34172/ajmb.2527 [Crossref] [ Google Scholar]
- Addissouky TA, Ali MM, El Sayed IE, Wang Y. Type 1 diabetes mellitus: retrospect and prospect. Bull Natl Res Cent 2024; 48(1):42. doi: 10.1186/s42269-024-01197-z [Crossref] [ Google Scholar]
- Yi X, Gao J, Wang Z. The human lung microbiome-A hidden link between microbes and human health and diseases. Imeta 2022; 1(3):e33. doi: 10.1002/imt2.33 [Crossref] [ Google Scholar]
- Chen Y, Fan LC, Chai YH, Xu JF. Advantages and challenges of metagenomic sequencing for the diagnosis of pulmonary infectious diseases. Clin Respir J 2022; 16(10):646-56. doi: 10.1111/crj.13538 [Crossref] [ Google Scholar]
- Agudelo-Pérez S, Fernández-Sarmiento J, Rivera León D, Peláez RG. Metagenomics by next-generation sequencing (mNGS) in the etiological characterization of neonatal and pediatric sepsis: a systematic review. Front Pediatr 2023; 11:1011723. doi: 10.3389/fped.2023.1011723 [Crossref] [ Google Scholar]
- Amrouche T, Chikindas ML. Probiotics for immunomodulation in prevention against respiratory viral infections with special emphasis on COVID-19. AIMS Microbiol 2022; 8(3):338-56. doi: 10.3934/microbiol.2022024 [Crossref] [ Google Scholar]
- Corriero A, Gadaleta RM, Puntillo F, Inchingolo F, Moschetta A, Brienza N. The central role of the gut in intensive care. Crit Care 2022; 26(1):379. doi: 10.1186/s13054-022-04259-8 [Crossref] [ Google Scholar]
- Marzaman AN, Roska TP, Sartini S, Utami RN, Sulistiawati S, Enggi CK. Recent advances in pharmaceutical approaches of antimicrobial agents for selective delivery in various administration routes. Antibiotics (Basel) 2023; 12(5):822. doi: 10.3390/antibiotics12050822 [Crossref] [ Google Scholar]
- Mokrani D, Chommeloux J, Pineton de Chambrun M, Hékimian G, Luyt CE. Antibiotic stewardship in the ICU: time to shift into overdrive. Ann Intensive Care 2023; 13(1):39. doi: 10.1186/s13613-023-01134-9 [Crossref] [ Google Scholar]
- Stoian A, Bajko Z, Stoian M, Cioflinc RA, Niculescu R, Arbănași EM. The occurrence of acute disseminated encephalomyelitis in SARS-CoV-2 infection/vaccination: our experience and a systematic review of the literature. Vaccines (Basel) 2023; 11(7):1225. doi: 10.3390/vaccines11071225 [Crossref] [ Google Scholar]
- She J, Hou D, Chen C, Bi J, Song Y. Challenges of vaccination and herd immunity in COVID-19 and management strategies. Clin Respir J 2022; 16(11):708-16. doi: 10.1111/crj.13543 [Crossref] [ Google Scholar]
- Luyt CE, Bouadma L, Morris AC, Dhanani JA, Kollef M, Lipman J. Pulmonary infections complicating ARDS. Intensive Care Med 2020; 46(12):2168-83. doi: 10.1007/s00134-020-06292-z [Crossref] [ Google Scholar]
- Gopal G, Muralidar S, Kamalakkannan A, Ambi SV. Microbiome in Acute Respiratory Distress Syndrome (ARDS). In: Gupta G, Oliver BG, Dua K, Singh A, MacLoughlin R, editors. Microbiome in Inflammatory Lung Diseases. Singapore: Springer Nature Singapore; 2022. p. 117-34. doi: 10.1007/978-981-16-8957-4_8.
- Addissouky TA, Ali MM, El Sayed IE, Wang Y. Recent advances in diagnosing and treating Helicobacter pylori through botanical extracts and advanced technologies. Arch Pharmacol Ther 2023; 5(1):53-66. doi: 10.33696/Pharmacol.4.045 [Crossref] [ Google Scholar]
- Fei Q, Bentley I, Ghadiali SN, Englert JA. Pulmonary drug delivery for acute respiratory distress syndrome. Pulm Pharmacol Ther 2023; 79:102196. doi: 10.1016/j.pupt.2023.102196 [Crossref] [ Google Scholar]
- Jiang L, Guo P, Ju J, Zhu X, Wu S, Dai J. Inhalation of L-arginine-modified liposomes targeting M1 macrophages to enhance curcumin therapeutic efficacy in ALI. Eur J Pharm Biopharm 2023; 182:21-31. doi: 10.1016/j.ejpb.2022.11.017 [Crossref] [ Google Scholar]
- Russell P, Esser L, Hagemeyer CE, Voelcker NH. The potential impact of nanomedicine on COVID-19-induced thrombosis. Nat Nanotechnol 2023; 18(1):11-22. doi: 10.1038/s41565-022-01270-6 [Crossref] [ Google Scholar]
- Areny-Balagueró A, Solé-Porta A, Camprubí-Rimblas M, Campaña-Duel E, Ceccato A, Roig A. Bioengineered extracellular vesicles: future of precision medicine for sepsis. Intensive Care Med Exp 2023; 11(1):11. doi: 10.1186/s40635-023-00491-w [Crossref] [ Google Scholar]
- Chen X, Xu J, Ji B, Fang X, Jin K, Qian J. The role of nanotechnology-based approaches for clinical infectious diseases and public health. Front Bioeng Biotechnol 2023; 11:1146252. doi: 10.3389/fbioe.2023.1146252 [Crossref] [ Google Scholar]
- Bittner E, Sheridan R. Acute respiratory distress syndrome, mechanical ventilation, and inhalation injury in burn patients. Surg Clin North Am 2023; 103(3):439-51. doi: 10.1016/j.suc.2023.01.006 [Crossref] [ Google Scholar]
- Addissouky TA, El Sayed IE, Ali MM, Wang Y. Emerging biomarkers for precision diagnosis and personalized treatment of cystic fibrosis. J Rare Dis 2024; 3(1):28. doi: 10.1007/s44162-024-00052-z [Crossref] [ Google Scholar]
- Battaglini D, Pelosi P, Robba C. Ten rules for optimizing ventilatory settings and targets in post-cardiac arrest patients. Crit Care 2022; 26(1):390. doi: 10.1186/s13054-022-04268-7 [Crossref] [ Google Scholar]
- Ramirez-Estrada S, Peña-Lopez Y, Vieceli T, Rello J. Ventilator-associated events: from surveillance to optimizing management. J Intensive Med 2023; 3(3):204-11. doi: 10.1016/j.jointm.2022.09.004 [Crossref] [ Google Scholar]
- Wang F, Chen M, Ma J, Wang C, Wang J, Xia H. Integrating bulk and single-cell sequencing reveals the phenotype-associated cell subpopulations in sepsis-induced acute lung injury. Front Immunol 2022; 13:981784. doi: 10.3389/fimmu.2022.981784 [Crossref] [ Google Scholar]
- Addissouky TA. Precision medicine for personalized cholecystitis care: integrating molecular diagnostics and biotherapeutics. Bull Natl Res Cent 2024; 48(1):89. doi: 10.1186/s42269-024-01244-9 [Crossref] [ Google Scholar]
- Battaglini D, Fazzini B, Silva PL, Cruz FF, Ball L, Robba C. Challenges in ARDS definition, management, and identification of effective personalized therapies. J Clin Med 2023; 12(4):1381. doi: 10.3390/jcm12041381 [Crossref] [ Google Scholar]
- Addissouky TA, El Sayed IE, Ali MM, Wang Y, El Baz A, Elarabany N. Oxidative stress and inflammation: elucidating mechanisms of smoking-attributable pathology for therapeutic targeting. Bull Natl Res Cent 2024; 48(1):16. doi: 10.1186/s42269-024-01174-6 [Crossref] [ Google Scholar]
- Ahmadi Marzaleh M, Peyravi M, Mousavi S, Sarpourian F, Seyedi M, Shalyari N. Artificial intelligence functionalities during the COVID-19 pandemic. Disaster Med Public Health Prep 2023; 17:e336. doi: 10.1017/dmp.2023.3 [Crossref] [ Google Scholar]
- Song Y, Lin W, Zhu W. Traditional Chinese medicine for treatment of sepsis and related multi-organ injury. Front Pharmacol 2023; 14:1003658. doi: 10.3389/fphar.2023.1003658 [Crossref] [ Google Scholar]
- Osuru HP, Ikeda K, Atluri N, Thiele RH. Moderate exercise-induced dynamics on key sepsis-associated signaling pathways in the liver. Crit Care 2023; 27(1):266. doi: 10.1186/s13054-023-04551-1 [Crossref] [ Google Scholar]
- Shashikumar SP, Wardi G, Malhotra A, Nemati S. Artificial intelligence sepsis prediction algorithm learns to say “I don’t know”. npj Digital Medicine 2021; 4(1):134. doi: 10.1038/s41746-021-00504-6 [Crossref] [ Google Scholar]
- Shashikumar SP, Wardi G, Malhotra A, Nemati S. Artificial intelligence sepsis prediction algorithm learns to say “I don’t know”. NPJ Digit Med 2021; 4(1):134. doi: 10.1038/s41746-021-00504-6 [Crossref] [ Google Scholar]
- Shah N, Arshad A, Mazer MB, Carroll CL, Shein SL, Remy KE. The use of machine learning and artificial intelligence within pediatric critical care. Pediatr Res 2023; 93(2):405-12. doi: 10.1038/s41390-022-02380-6 [Crossref] [ Google Scholar]
- Cascella M, Montomoli J, Bellini V, Bignami E. Evaluating the feasibility of ChatGPT in healthcare: an analysis of multiple clinical and research scenarios. J Med Syst 2023; 47(1):33. doi: 10.1007/s10916-023-01925-4 [Crossref] [ Google Scholar]