Avicenna Journal of Clinical Microbiology and Infection. 12(3):115-120.
doi: 10.34172/ajcmi.3647
Original Article
Prevalence, Etiology, and Antimicrobial Resistance Pattern of Bacterial Isolates From Bloodstream Infections in Ganjavian Hospital, Dezful, Iran
Behnaz Deihim Conceptualization, Data curation, Investigation, Methodology, Writing – original draft, Writing – review & editing, 1, 2, * 
Ahmad Ali Assarian Formal analysis, Investigation, Writing – original draft, Writing – review & editing, 3
Mohammad Shoja Data curation, Writing – original draft, Writing – review & editing, 4
Author information:
1Infectious and Tropical Diseases Research Center, Dezful University of Medical Sciences, Dezful, Iran
2Department of Bacteriology and Virology, School of Medicine, Dezful University of Medical Sciences, Dezful, Iran
3Department of Infectious Diseases, School of Medicine, University of Medical Sciences, Dezful, Iran
4Student Research Committee, Dezful University of Medical Sciences, Dezful, Iran
Abstract
Background: Sepsis is a life-threatening condition with high mortality rates. The emergence of antimicrobial resistance (AMR) among pathogens that cause sepsis poses a significant challenge to effective treatment. This study was conducted to determine the AMR patterns of bacterial isolates from septic patients’ blood cultures with emphasis on extended-spectrum beta-lactamases (ESBLs), carbapenemase, and methicillin-resistant Staphylococcus aureus (MRSA) prevalence.
Methods: This cross-sectional laboratory study examined blood culture samples of 1248 patients. The blood cultures were subcultured on MacConkey and chocolate agar media. Bacterial identification was based on gram-staining and biochemical tests. Initial and confirmatory antibiotic susceptibility testing was then performed according to CLSI 2022 for MRSA, vancomycin-resistant Enterococcus (VRE), and ESBLs. The statistical analysis of the study findings was conducted using SPSS. The accuracy level of the evaluations was determined with a 95% confidence interval.
Results: Among the 174 cases of bloodstream infection (BSI) (13.9% positivity), Enterobacterales (59.8%) and gram-positive cocci (32.7%) were dominant isolates. Interestingly, the prevalence of MRSA was 67.5%, with a significantly higher prevalence in ICUs (81.3%; P=0.037). In gram-negative isolates, resistance to third-generation cephalosporins and carbapenems was 48.7% and 22.2%, respectively. Significant resistance to carbapenems (80%) was observed in Acinetobacter isolates, but all strains remained susceptible to colistin. ESBL producers included Escherichia coli (36.3%) and Klebsiella pneumoniae (16%). Notably, 52.4% of multidrug-resistant Enterobacteriaceae cases were isolated from patients in emergency departments and intensive care units.
Conclusion: This study highlights the alarming prevalence of MDR bacteria among sepsis isolates. Precautions should be taken against this growing threat by focusing on three priorities: enhancing infection control, maintaining continuous surveillance, and exploring novel therapeutic approaches.
Keywords: Blood culture, Antibiotic resistance, ESBL, MRSA, VRE
Copyright and License Information
© 2025 The Author(s); Published by Hamadan University of Medical Sciences.
This is an open-access article distributed under the terms of the Creative Commons Attribution License (
https://creativecommons.org/licenses/by/4.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Please cite this article as follows: Deihim B, Assarian AA, Shoja M. Prevalence, etiology, and antimicrobial resistance pattern of bacterial isolates from bloodstream infections in Ganjavian hospital, Dezful, Iran. Avicenna J Clin Microbiol Infect. 2025;12(3):115-120. doi:10.34172/ajcmi.3647
Introduction
Sepsis, a life-threatening systemic response to infection, claims millions of lives annually. In 2020, there were approximately 48.9 million global sepsis cases, resulting in 11 million deaths (nearly 1 in 5 global fatalities). Even more alarming, the incidence of sepsis has risen steadily worldwide over the past two decades (1,2). Key factors include: aging populations, immunocompromising conditions, increased prevalence of chronic comorbidities, and suboptimal antibiotic use (e.g., inappropriate treatment protocols or incomplete courses). These prescribing errors inadvertently train bacteria to become drug-resistant superbugs (3).
For bloodstream infections (BSIs), every minute counts; in other words, delaying appropriate antimicrobial therapy significantly increases the risk of mortality. Initial empirical therapies (based on informed guidelines) may take several days to show their effects (4). Surprisingly, sepsis can arise from pneumonia, urinary tract infections, or even skin wounds. In recent decades, evolving pathogens, including Escherichia coli, Klebsiella pneumoniae, Pseudomonas aeruginosa, and Acinetobacter baumannii, especially extended-spectrum and metallo-beta-lactamase-producing strains, as well as methicillin- and vancomycin-resistant Staphylococcus aureus (MRSA and VRSA) and vancomycin-resistant Enterococcus (VRE), have become a growing crisis for healthcare systems due to their rising resistance to last-line drugs (5).
Effective antimicrobial therapy for infectious diseases depends on precise pathogen identification and antimicrobial susceptibility testing to optimize treatment, minimize unnecessary antibiotic use, and protect the commensal microbiota. Although empirical therapy remains critical for severe infections, the rising threat of antimicrobial resistance (AMR) is diminishing its efficacy. Consequently, laboratory diagnostics are crucial for detecting resistant pathogens, informing evidence-based treatment decisions, and preventing the spread of resistance. Nevertheless, diagnostic challenges often delay optimal therapy, exacerbating both clinical outcomes and public health risks (6).
AMR is a significant global health threat, particularly in BSIs, where delays in effective treatment lead to high mortality rates. Accurate epidemiological data and regional antibiotic resistance patterns are critical for appropriate antibiotic prescribing. AMR leads to multiple negative consequences, including increased complications, prolonged hospital stays, and higher rates of therapeutic failures. This crisis is exacerbated in developing countries due to inadequate surveillance, poor infection control practices, overuse of antibiotics, and limited access to newer therapies (7). Therefore, active monitoring of resistance trends is essential for guiding responsible antibiotic use and stewardship programs (8). Understanding the prevalence and resistance patterns of BSIs in hospitalized patients is crucial to ensure timely and effective antibiotic treatment. This study aimed to evaluate the prevalence, causative pathogens, and AMR profiles of bacterial BSIs in Ganjavian Hospital to inform therapeutic decisions and enhance infection control measures.
Materials and Methods
This descriptive cross-sectional study aimed to examine the antibiotic resistance profiles of bacteria isolated from blood culture samples collected from patients admitted to Ganjavian Hospital in 2022. Sequential sampling was used to include all patients suspected of sepsis.
In the current study, blood culture bottles were subcultured on days 1, 3, and 6 onto chocolate agar and MacConkey agar media (Condalab, Spain) at 35 °C for 18 hours to optimize microbial recovery of both early and late-growing pathogens. Following incubation, bacterial identification was carried out through a series of tests, including gram staining, catalase, oxidase, DNase, coagulase, Mannitol Salt Agar, Bile Esculin Agar, CAMP (Christie, Atkinson, Munch, Peterson) test, glucose Oxidizer-Fermenter reactions, and IMViC (Condalab) (9).
According to the distinguishing criteria for true BSIs from possible contamination, including common organisms associated with pseudobacteremia (coagulase-negative staphylococci, Corynebacterium species, and Bacillus species), we performed repeat blood cultures. According to the current diagnostic standards, only isolates that showed persistent growth in serial blood cultures were considered pathogenic. In our study, blood culture samples presenting this challenge were obtained from the pediatric department, where repeat cultures of initially positive samples for these organisms yielded negative results, confirming the contamination. Consequently, these cases were excluded from the final analysis of BSI prevalence (10,11).
For antimicrobial susceptibility testing, a bacterial suspension was prepared to match the turbidity of the 0.5 McFarland standard and inoculated on Mueller-Hinton agar (MHA) (Condalab, Madrid, Spain). The test was performed using the Kirby-Bauer disk diffusion method for various antibiotics, including amikacin (30 µg), gentamicin (10 µg), imipenem (10 µg), meropenem (10 µg), cefotaxime (30 µg), ceftriaxone (30 µg), ciprofloxacin (5 µg), trimethoprim-sulfamethoxazole (1.25/23.75 µg), piperacillin-tazobactam (100/10 µg), ampicillin (10 µg), penicillin (10 units), erythromycin (15 µg), tetracycline (30 µg), clindamycin (2 µg), linezolid (30 µg), rifampin (5 µg), and vancomycin (30 µg) (MAST Company). Antibiotic susceptibility was determined by measuring the growth inhibition zones and interpreting according to the Clinical and Laboratory Standards Institute (CLSI) 2022 M100 (32nd edition) guidelines (12).
Cefoxitin (30 µg) was used to detect methicillin-resistant S. aureus (MRSA). Vancomycin resistance in Enterococcus and Staphylococcus was evaluated using the Vancomycin Agar test, and the minimal inhibitory concentration (MIC) (0.016 to 256 μg/mL) was determined by Etest assay (Liofilchem). To detect extended-spectrum beta-lactamase (ESBL) and carbapenemase production in Enterobacteriaceae and Pseudomonas, ceftazidime (CAZ) combined with clavulanic acid and modified carbapenem inactivation method (mCIM) was used, respectively. Additionally, the EDTA-modified carbapenem inactivation method (eCIM) and mCIM tests were simultaneously used to differentiate between serine carbapenemase and metallo-beta-lactamase resistance. Colistin resistance was determined based on CLSI guidelines, with an MIC value of ≥ 4 μg/mL indicating resistance (12).
The statistical analysis of study findings was conducted using IBM SPSS version 21.0. The chi-square and Fisher’s exact test were used for comparisons. Categorical variables were analyzed with a predetermined significance level of P < 0.05 and 95% confidence intervals.
Results
Demographics
Bacterial growth was detected in 174 (13.9%) of 1248 blood cultures. Among these isolates, 89 (51.1%) belonged to male patients and 85 (48.9%) belonged to female patients. The age of the patients ranged from 1 day to 89 years. Most cultures were collected in the emergency department (n = 494, 39.6%), followed by intensive care units (ICUs), internal medicine, and surgical departments, which accounted for 31.6% (n = 394), 25.3% (n = 316), and 3.5% (n = 44), respectively.
Distribution of Bacteria
Microbiological analysis revealed that the frequency of gram-positive cocci was 32.7% (57/174) and the frequency of Enterobacterales was 59.8% (104/174) of the isolates. Additionally, non-fermenting bacteria, including P. aeruginosa and A. baumannii, were isolated in 7.5% (13/174). The most frequently isolated pathogens were E. coli (25.3%), S. aureus (23%), and K. pneumoniae (14.4%).
Resistance Profiles
Staphylococcus aureus isolates exhibited the highest resistance rates to ampicillin and tetracycline, while vancomycin and linezolid showed the greatest efficacy. Clindamycin resistance was observed in 22.5% (9/40) of strains, with an MRSA prevalence of 67.5% (27/40). No vancomycin resistance was detected among S. aureus isolates using vancomycin agar and MIC testing (MIC range: 0.125-1.5 μg/mL). A significant association emerged between the prevalence of MRSA and hospital wards (P = 0.037), particularly in ICUs, where 81.3% of S. aureus isolates were MRSA. Fisher’s exact test revealed no association between MRSA occurrence and patient gender (P = 0.107).
Enterococcus isolates (n = 11) comprised E. faecalis (27.3%, n = 3) and E. faecium (72.7%, n = 8). All isolates demonstrated ciprofloxacin resistance, while 36.4% (n = 4) of isolates were vancomycin-resistant enterococci (VRE) (MIC > 256 μg/mL). No significant associations were found between VRE prevalence and gender or hospital departments (P > 0.05).
Gram-negative bacteria (n = 117) showed 48.7% (n = 57) resistance to third-generation cephalosporins. Among the 104 isolates of Enterobacterales, 21 strains (20.1%) were multiple-drug resistant (MDR), predominantly from emergency (52.4%, n = 11) and ICU (23.8%, n = 5). ESBL production was identified in 20 strains (E. coli: 36.3%, n = 16; K. pneumoniae: 16%, n = 4).
Eight isolates of A. baumannii were isolated from ICU patients, which demonstrated the highest level of antibiotic resistance. The rate of multidrug-resistant A. baumannii (MDR-AB) was 87.5% (7/8), with all strains showing susceptibility to colistin as indicated by the Colistin E-Test. Following colistin, piperacillin-tazobactam was the next most effective antibiotic against A. baumannii, with 37% (3/8) susceptibility.
In our research, 5 strains of P. aeruginosa were isolated. Four strains exhibited sensitivity to ciprofloxacin, gentamicin, cotrimoxazole, and third-generation cephalosporins, and 3 isolates demonstrated resistance to meropenem and amikacin.
Figure 1 illustrates the patterns of antibiotic resistance among gram-negative isolates. Furthermore, carbapenem resistance rates in Enterobacterales, P. aeruginosa, and A. baumannii were 16.3% (17/104), 40% (2/5), and 87.5% (7/8), respectively. Carbapenemase production was detected in 14.4% (15/104) of Enterobacterales and 40% (2/5) of P. aeruginosa isolates using the modified carbapenem inactivation method (mCIM). The investigation examined the production of serine carbapenemases and metallo-beta-lactamases through the simultaneous use of mCIM and eCIM methods. Serine carbapenemase production among Enterobacterales isolates was distributed as follows: E. coli (2.3%), K. pneumoniae (32%), K. oxytoca (11.1%), and K. aerogenes (25%).Only 2 Klebsiella strains produced metallo-beta-lactamases. No significant associations were found between carbapenem resistance and gender/ward distribution (P < 0.05). Three isolates (1 K. pneumoniae, 1 K. aerogenes, and 1 P. aeruginosa) were categorized as intermediate (MIC > 2 μg/mL) according to CLSI guidelines, while all others remained susceptible.
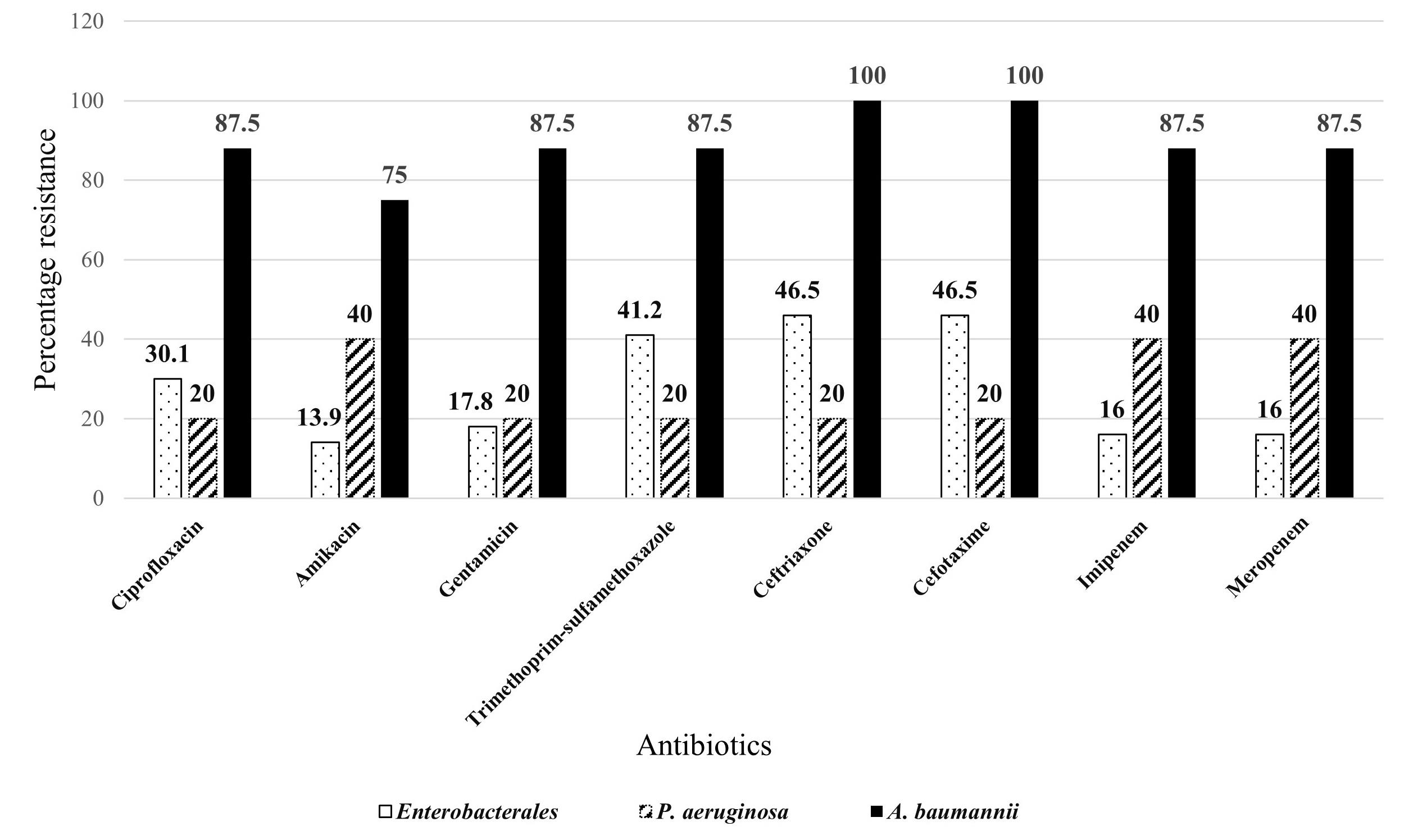
Figure 1.
Antibiotic-Resistance Pattern of Gram-Negative Bacteria by Disk Diffusion Method
.
Antibiotic-Resistance Pattern of Gram-Negative Bacteria by Disk Diffusion Method
Discussion
The increasing prevalence of antibiotic resistance is a significant challenge for health systems worldwide. Region-specific data on antibiotic resistance patterns is crucial for effective treatment, especially in critical care, due to its increasing prevalence. In this study, bacterial infections accounted for 13.9% of positive blood cultures, with E. coli (25.3%), S. aureus (23%), and K. pneumoniae (14.4%) being the predominant isolates. While these results align with the results of the study by Oyekale et al (13) (E. coli: 29.4%), they contrast with the findings of the study conducted by Mohammadi et al (14), who reported S. aureus (31.5%) as most common, and Mahmoudi et al (15), who identified coagulase-negative staphylococci and Proteus vulgaris as prevalent pathogens. These variations may stem from differences in diagnostic methods (e.g., automated systems like BacTec/MALDI-TOF vs. conventional techniques) (16), as limited access to advanced tools persists in many settings (17).
Consistent with studies from Shiraz (17) (63.3%) and other places (18,19), gram-negative bacteria dominated (67.3%), though Abayneh et al (18) found no significant differences in the frequency of gram-positive or Enterobacteriaceae. These findings underscore the need for region-specific resistance monitoring and standardized diagnostics to optimize treatment strategies.
Moradi reported a higher prevalence of positive blood cultures among emergency department patients (60.4%) compared to our findings (52.4%), highlighting the notable frequency of such cases in emergency settings (20). The observed overrepresentation of positive blood cultures among emergency department patients can be attributed to the standardized practice of obtaining blood cultures upon admission before initiating antibiotic therapy (21). This routine procedure, prevalent in emergency settings, likely contributes to the higher isolation rates identified in our study compared to those reported in studies focusing on intensive care unit patients. The absence of a dedicated infectious diseases department may have further influenced these findings.
Our study revealed an ESBL prevalence of 21.5% among Enterobacterales, which aligns with the study by Bandy (22) but demonstrates notably lower rates than those reported in China (23). This geographical variation is particularly evident when comparing specific pathogens. In our study, E. coli (36.3%) and K. pneumoniae (16%) emerged as key ESBL producers, whereas in the study by Amanati et al (24), substantially higher rates were documented (66.7% and 60.7%, respectively). These differences highlight the importance of localized resistance monitoring for clinical practice.
The extreme resistance observed in Acinetobacter requires an urgent revision of our region’s empirical treatment guidelines. Prolonged hospitalizations, the use of invasive devices, and overprescription of antibiotics exacerbate gram-negative resistance, creating selection pressure that fuels resistance cycles (25). The susceptibility of immunocompromised patients and the occurrence of healthcare-associated transmission underscore the urgent need for enhanced infection control and coordinated antimicrobial stewardship. Carbapenems and colistin remain among the most critical last-line antibiotics for treating multidrug-resistant infections. Our findings revealed alarming resistance patterns, particularly among A. baumannii isolates, which showed complete resistance to cephalosporins and 87.5% resistance to carbapenems, exceeding previously reported rates (26). Interestingly, while regional studies reported colistin resistance rates of 13.6% in Enterobacteriaceae (27) and 13.4% in A. baumannii (28), we detected no colistin-resistant strains. However, carbapenemase resistance (14.6%) and metallo-beta-lactamase resistance (2.2%) were present, as confirmed by mCIM/eCIM testing. The rate of carbapenem resistance in our study showed significant interspecies variation. The overall rate of resistance among gram-negative isolates (22.2%) was closely consistent with the findings reported by Balkhair et al (27.7%) (29) in Oman, indicating similar regional resistance patterns. This is particularly concerning given its association with a three-fold increase in 30-day mortality. Nasiri et al (30) reported carbapenem resistance of 24% in K. pneumoniae and 5% in E. coli. Although resistance patterns differ regionally, the broader trend remains clear. In other words, resistance to carbapenem and colistin is an escalating threat.
Our study found E. coli (25.3%) and S. aureus (23%) to be the most prevalent pathogens. These findings align with those of Maham et al (31) and Pourakbari et al (32), who reported similar challenges with MRSA. Specifically, we observed a high frequency of MRSA (67.5%) and VRE (36.4%), consistent with the study by Besharati et al (33). In contrast to the report by Mohammadi et al (14), all of our isolates remained susceptible to vancomycin. However, widespread resistance to older antibiotics, such as ampicillin (82%), erythromycin (75%), and tetracycline (68%), suggests that these agents may no longer be reliable for empirical therapy. These findings emphasize the importance of vancomycin as a critical therapeutic option, particularly for MRSA infections. Notably, we found no association between MRSA prevalence and patient gender (P = 0.107), contradicting studies that propose demographic risk factors. These discrepancies may reflect regional variations in antibiotic prescribing practices or infection control measures.
Our observation of 100% resistance to ciprofloxacin and erythromycin among enterococci aligns with trends noted by Shokoohizadeh et al (34). The high rates of resistance to penicillin and ampicillin among enterococci isolates (54%) observed in our region align with broader AMR trends, underscoring the urgent need for continuous local surveillance and the implementation of targeted therapeutic protocols. Our findings, supported by An et al (35), reveal that the prevalence of MRSA varies significantly across geographic regions, highlighting the importance of having access to regional data for clinical decision-making.
This study has several limitations worth acknowledging. First, the reliance on phenotypic methods without complementary molecular testing (e.g., PCR or whole-genome sequencing) precluded the identification of specific genetic resistance determinants. Second, although our sample size (n = 1248) provided meaningful data, expanding to multiple centers may improve the detection of rare resistance patterns. Nevertheless, our findings provided important insights into regional AMR trends in BSIs, including: (1) high ESBL prevalence, (2) alarming MRSA rates in ICUs (81.3%), (3) emerging carbapenem resistance in A. baumannii (87.5%), and (4) preserved colistin susceptibility across all isolates. Future multicenter studies incorporating genotypic characterization are needed to validate these trends and guide regional infection control strategies.
In response to these challenges, it is crucial to support infection prevention and control practices in our hospital. This includes rigorous hand hygiene, appropriate use of invasive devices, continuous monitoring of disinfection processes, and immediate isolation of patients with multidrug-resistant organisms. An effective surveillance program will enable early detection of resistance patterns and facilitate necessary interventions, ultimately limiting the spread of resistant pathogens.
Conclusion
The high prevalence of multidrug-resistant organisms (ESBL-producing Enterobacteriaceae, MRSA, and VRE) in our hospital could have serious clinical and economic consequences. Based on AMR patterns detected in the current study, we propose the following evidence-based hospital-specific interventions. AMR surveillance systems should be strengthened by implementing active screening for resistant strains in high-risk wards. Targeted surveillance programs should be implemented to educate physicians to limit unnecessary antibiotic prescribing. Advanced infection control measures should include reducing contact precautions for carriers of MDR pathogens and monitoring hand hygiene. This triad, supported by lab-clinician collaboration, can effectively combat drug resistance while preserving the therapeutic options.
Acknowledgments
The authors thank the Infectious and Tropical Diseases Research Center, Dezful University of Medical Sciences, Dezful, Iran, for their support, cooperation, and assistance throughout the study (Grant number: MED-400054-1400).
Competing Interests
The authors have no conflicts of interest to declare.
Ethical Aproval
Ethical committee approval received from the Ethics Committee of Dezful University of Medical Sciences (Approval no: IR.DUMS.REC.1401.002).
Funding
This article is part of the General Physician thesis, financially supported by the Faculty of Medicine, Dezful University of Medical Sciences (Grant number: MED-400075-1400). We received funding for this article from the vice chancellor of research at Dezful University of Medical Sciences.
References
- Fleischmann-Struzek C, Rudd K. Challenges of assessing the burden of sepsis. Med Klin Intensivmed Notfmed 2023; 118(Suppl 2):68-74. doi: 10.1007/s00063-023-01088-7 [Crossref] [ Google Scholar]
- Rudd KE, Johnson SC, Agesa KM, Shackelford KA, Tsoi D, Kievlan DR. Global, regional, and national sepsis incidence and mortality, 1990-2017: analysis for the Global Burden of Disease Study. Lancet 2020; 395(10219):200-11. doi: 10.1016/s0140-6736(19)32989-7 [Crossref] [ Google Scholar]
- Quiros-Roldan E, Sottini A, Natali PG, Imberti L. The impact of immune system aging on infectious diseases. Microorganisms 2024; 12(4):775. doi: 10.3390/microorganisms12040775 [Crossref] [ Google Scholar]
- Ji J, Klaus J, Burnham JP, Michelson A, McEvoy CA, Kollef MH. Bloodstream infections and delayed antibiotic coverage are associated with negative hospital outcomes in hematopoietic stem cell transplant recipients. Chest 2020; 158(4):1385-96. doi: 10.1016/j.chest.2020.06.011 [Crossref] [ Google Scholar]
- Hosseini MB, Abdoli Oskouei S, Heidari F, Sadat Sharif A, Salimi Z, Sharif SA. Determination of the frequency of microbial agents and drug susceptibility pattern of the neonatal sepsis in the neonatal intensive care unit at Alzahra hospital, Tabriz, Iran. Iran J Neonatol 2019; 10(4):33-40. doi: 10.22038/ijn.2019.37288.1574 [Crossref] [ Google Scholar]
- Khalid M. The role of the clinical microbiology laboratory in improving antimicrobial stewardship: systematic review. J Clin Lab Sci Technol 2022; 1(1):1-7. doi: 10.56546/jclsts.v1i1.2 [Crossref] [ Google Scholar]
- Kumar NR, Balraj TA, Kempegowda SN, Prashant A. Multidrug-resistant sepsis: a critical healthcare challenge. Antibiotics (Basel) 2024; 13(1):46. doi: 10.3390/antibiotics13010046 [Crossref] [ Google Scholar]
- Yamin D, Uskoković V, Wakil AM, Goni MD, Shamsuddin SH, Mustafa FH. Current and future technologies for the detection of antibiotic-resistant bacteria. Diagnostics (Basel) 2023; 13(20):3246. doi: 10.3390/diagnostics13203246 [Crossref] [ Google Scholar]
- Forbes BA, Sahm DF, Weissfeld AS. Bailey and Scotts’ Diagnostic Microbiology. 15th ed. St Louis: Mosby; 2021. p. 322.
- Jameson JL, Fauci AS, Kasper DL, Hauser SL, Longo DL, Loscalzo J. Harrison’s Principles of Internal Medicine. 20th ed. New York: McGraw-Hill; 2018.
- Murni IK, Duke T, Daley AJ, Kinney S, Soenarto Y. True pathogen or contamination: validation of blood cultures for the diagnosis of nosocomial infections in a developing country. J Trop Pediatr 2018; 64(5):389-94. doi: 10.1093/tropej/fmx081 [Crossref] [ Google Scholar]
- Clinical and Laboratory Standards Institute (CLSI). Performance Standards for Antimicrobial Susceptibility Testing. 32nd ed. CLSI Supplement M100. Wayne, PA: CLSI; 2022.
- Oyekale OT, Ojo BO, Olajide AT, Oyekale OI. Bacteriological profile and antibiogram of blood culture isolates from bloodstream infections in a rural tertiary hospital in Nigeria. Afr J Lab Med 2022; 11(1):1807. doi: 10.4102/ajlm.v11i1.1807 [Crossref] [ Google Scholar]
- Mohammadi F, Moshirpanahi Aliabad D, Razzaghi M, Hoseinzadeh E, Doosti Irani A. Frequency and pattern of bacterial antibiotic resistance in blood culture samples of hospitalized patients in Besat hospital in Hamadan (2010-2020). Avicenna J Clin Med 2022; 29(2):102-9. doi: 10.32592/ajcm.29.2.102 [Crossref] [ Google Scholar]
- Mahmoudi H, Ghasemi Bassir HR, Hosseini SM, Arabestani MR, Alikhani MY. The frequency of bacteria isolated from blood cultures and antibiotic susceptibility patterns among admitted patients in hospital of Hamedan University of Medical Sciences. Iran J Med Microbiol 2016; 10(4):69-74. [ Google Scholar]
- Wang Y, Jin Y, Bai Y, Song Z, Chu W, Zhao M. Rapid method for direct identification of positive blood cultures by MALDI-TOF MS. Exp Ther Med 2020; 20(6):235. doi: 10.3892/etm.2020.9365 [Crossref] [ Google Scholar]
- Amin Shahidi M, Anvarinejad M, Abbasian A, Abbasi P, Rafaatpour N, Dehyadegari MA, et al. Characterization of multi-drug resistant ESBL producing nonfermenter bacteria isolated from patients blood samples using phenotypic methods in Shiraz (Iran). J Birjand Univ Med Sci 2015;22(3):256-65. [Persian].
- Abayneh M, Hailemariam S, Asnake M. Bacterial profile and multi-drug resistance pattern of bacterial isolates among septicemia suspected cases: a meta-analysis report in Ethiopia. J Lab Med 2021; 45(3):167-78. doi: 10.1515/labmed-2020-0124 [Crossref] [ Google Scholar]
- Manyahi J, Kibwana U, Mgimba E, Majigo M. Multi-drug resistant bacteria predict mortality in bloodstream infection in a tertiary setting in Tanzania. PLoS One 2020; 15(3):e0220424. doi: 10.1371/journal.pone.0220424 [Crossref] [ Google Scholar]
- Moradi N, Javadpoor S, Vahdani M. Prevalence and antibiogram pattern of gram-negative bacteria isolated from blood cultures in Shahid Mohammadi Hospital Bandar Abbas. J Prevent Med 2015;2(2):55-61. [Persian].
- Hirosawa T, Sakamoto T, Hanai S, Harada Y, Shimizu T. Effect of prior antibiotic treatment on blood culture in an outpatient department of general internal medicine: a retrospective case-control analysis. Int J Gen Med 2023; 16:2709-17. doi: 10.2147/ijgm.S416235 [Crossref] [ Google Scholar]
- Bandy A, Tantry B. ESBL activity, MDR, and carbapenem resistance among predominant Enterobacterales isolated in 2019. Antibiotics (Basel) 2021; 10(6):744. doi: 10.3390/antibiotics10060744 [Crossref] [ Google Scholar]
- Yan M, Zheng B, Li Y, Lv Y. Antimicrobial susceptibility trends among gram-negative bacilli causing bloodstream infections: results from the China antimicrobial resistance surveillance trial (CARST) program, 2011-2020. Infect Drug Resist 2022; 15:2325-37. doi: 10.2147/idr.S358788 [Crossref] [ Google Scholar]
- Amanati A, Sajedianfard S, Khajeh S, Ghasempour S, Mehrangiz S, Nematolahi S. Bloodstream infections in adult patients with malignancy, epidemiology, microbiology, and risk factors associated with mortality and multi-drug resistance. BMC Infect Dis 2021; 21(1):636. doi: 10.1186/s12879-021-06243-z [Crossref] [ Google Scholar]
- Tacconelli E. Linking infection control to clinical management of infections to overcome antimicrobial resistance. J Hosp Infect 2021; 114:1-9. doi: 10.1016/j.jhin.2021.04.030 [Crossref] [ Google Scholar]
- Deihim B, Khorramizadeh M. Phenotypic and molecular detection of Acinetobacter baumannii strains producing carbapenemase from clinical specimens in Dezful teaching hospital. Majalah Kedokt Bandung 2024; 56(4):235-43. doi: 10.15395/mkb.v56.3794 [Crossref] [ Google Scholar]
- Moosavian M, Emam N. The first report of emerging mobilized colistin-resistance (MCR) genes and ERIC-PCR typing in Escherichia coli and Klebsiella pneumoniae clinical isolates in southwest Iran. Infect Drug Resist 2019; 12:1001-10. doi: 10.2147/idr.S192597 [Crossref] [ Google Scholar]
- Keramat F, Ghasemi Basir HR, Taher A, Moradi A, Saadatmand A, Owji Nejad P. Evaluation of antibiotic resistance to colistin in nosocomial infections with multidrug-resistant Acinetobacter. Avicenna J Clin Med 2021; 27(4):211-6. doi: 10.52547/ajcm.27.4.211 [Crossref] [ Google Scholar]
- Balkhair A, Saadi KA, Adawi BA. Epidemiology and mortality outcome of carbapenem- and colistin-resistant Klebsiella pneumoniae, Escherichia coli, Acinetobacter baumannii, and Pseudomonas aeruginosa bloodstream infections. IJID Reg 2023; 7:1-5. doi: 10.1016/j.ijregi.2023.01.002 [Crossref] [ Google Scholar]
- Nasiri MJ, Mirsaeidi M, Mousavi SM, Arshadi M, Fardsanei F, Deihim B. Prevalence and mechanisms of carbapenem resistance in Klebsiella pneumoniae and Escherichia coli: a systematic review and meta-analysis of cross-sectional studies from Iran. Microb Drug Resist 2020; 26(12):1491-502. doi: 10.1089/mdr.2019.0440 [Crossref] [ Google Scholar]
- Maham S, Fallah F, Gholinejad Z, Seifi A, Hoseini-Alfatemi SM. Bacterial etiology and antibiotic resistance pattern of pediatric bloodstream infections: a multicenter based study in Tehran, Iran. Ann Ig 2018; 30(4):337-45. doi: 10.7416/ai.2018.2225 [Crossref] [ Google Scholar]
- Pourakbari B, Mahmoudi S, Moradzadeh M, Mahzari M, Haghi Ashtiani MT, Tanzifi P. Antimicrobial resistance patterns of the gram-positive bacteria isolated from children with bloodstream infection in an Iranian referral hospital: a 6-year study. Infect Disord Drug Targets 2018; 18(2):136-44. doi: 10.2174/1871526517666170821164343 [Crossref] [ Google Scholar]
- Besharati R, Ghafouri M, Safamanesh S, Khosrojerdi M, Ghazvini K, Nojumi S. Molecular epidemiology of Panton-Valentine leukocidin harboring hospital-associated methicillin-resistant Staphylococcus aureus in septicemic children, northeastern Iran, Bojnurd. Jundishapur J Microbiol 2019; 12(2):e68183. doi: 10.5812/jjm.68183 [Crossref] [ Google Scholar]
- Shokoohizadeh L, Dehghani T, Namordizadeh V, Karmostaji A. New sequence types of Staphylococcus aureus strains isolated from hospitals and community settings in southern Iran. Jundishapur J Microbiol 2024; 17(2):e144398. doi: 10.5812/jjm-144398 [Crossref] [ Google Scholar]
- An NV, Nguyen HT, Nguyen Le V, Thu Van HT, Hai NM, Luong VH. Antimicrobial susceptibility profile of methicillin-resistant Staphylococcus aureus isolated from clinical samples at Bac Ninh Provincial General Hospital, Vietnam. Infect Drug Resist 2024; 17:4113-23. doi: 10.2147/idr.S477031 [Crossref] [ Google Scholar]