Avicenna Journal of Clinical Microbiology and Infection. 12(4):166-172.
doi: 10.34172/ajcmi.3641
Original Article
Antibiotic Resistance in Enterococcus Faecalis and Pseudomonas Aeruginosa Causing Urinary Infections in Central Vietnam
Nguyen Thi Doan Trinh Conceptualization, Data curation, Formal analysis, Funding acquisition, Project administration, Resources, Supervision, Visualization, Writing – original draft, Writing – review & editing, 1 
Truong Thi Thu Suong Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Resources, Software, Writing – original draft, Writing – review & editing, 1
Hoang Thi Minh Hoa Data curation, Methodology, Software, Validation, Visualization, Writing – review & editing, 1
Nguyen Huy Hoang Investigation, Methodology, Software, Validation, Visualization, Writing – review & editing, 1
Na T. D. Tran Conceptualization, Funding acquisition, Project administration, Resources, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing, 1, *
Author information:
1Department of Medical Laboratory Science, Da Nang University of Medical Technology and Pharmacy, Da Nang, Vietnam
Abstract
Background: Urinary tract infections (UTIs) are among the most common bacterial infections worldwide and are becoming increasingly complicated by the emergence of multidrug-resistant pathogens. Enterococcus faecalis and Pseudomonas aeruginosa are important pathogens of UTIs, particularly in hospitalized patients. Their rising resistance to multiple antibiotic classes poses a serious challenge to treatment and infection control, especially in low-income and middle-income countries, including Vietnam. Accordingly, this study aimed to determine the frequency of E. faecalis and P. aeruginosa in UTIs and assess their antibiotic-resistance status at Da Nang C Hospital, Central Vietnam, in 2022.
Methods: This retrospective cross-sectional study was conducted on 299 bacterial strains isolated from the urine specimens of patients diagnosed with UTIs at Da Nang C Hospital in 2022. These strains were identified through culture analysis, and their antibiotic susceptibility was assessed using the disk-diffusion method (Kirby-Bauer test).
Results: E. faecalis and P. aeruginosa were found in 10.03% and 8.7% of cultures, respectively. All isolates of E. faecalis were completely susceptible to linezolid, and most of them were susceptible to rifampin (93.8%) and vancomycin (86.2%). In addition, many of these isolates were susceptible to penicillin G, ampicillin, doxycycline, and chloramphenicol (67.9–77.8%). Resistance to ciprofloxacin, tetracycline, levofloxacin, and erythromycin was detected in 68–88.9% of isolates. Regarding P. aeruginosa, 53.8% to 66.7% of cultures were resistant to levofloxacin, gentamicin, ciprofloxacin, tobramycin, ofloxacin, and nitrofurantoin. However, P. aeruginosa was highly susceptible to piperacillin/tazobactam (87.5% of isolates), imipenem (75%), cefoperazone/sulbactam (72.7%), and cefepime and meropenem (64%). Eventually, multidrug resistance was observed in 56.7% and 34.6% of E. faecalis and P. aeruginosa isolates, respectively.
Conclusion: The bacteria isolated in this study exhibited resistance to many commonly used antibiotics at various levels. Our findings demonstrated the critical need for more stringent antibiotic stewardship guidelines and routine surveillance in order to enhance patient outcomes and prevent the spread of resistant bacteria.
Keywords: Enterococcus faecalis, Pseudomonas aeruginosa, Urinary tract infection, Antibiotic resistance
Copyright and License Information
© 2025 The Author(s); Published by Hamadan University of Medical Sciences.
This is an open-access article distributed under the terms of the Creative Commons Attribution License (
https://creativecommons.org/licenses/by/4.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Please cite this article as follows: Trinh NTD, Suong TTT, Hoa HHTM, Hoang NH, Tran NTD. Antibiotic resistance in Enterococcus faecalis and Pseudomonas aeruginosa causing urinary infections in central Vietnam. Avicenna J Clin Microbiol Infect. 2025;12(4):166-172. doi:10.34172/ajcmi.3641
Introduction
Urinary tract infections (UTIs) are prevalent among individuals of all ages worldwide. Enterococcus faecalis and Pseudomonas aeruginosa bacteria are common causes of these infections in Vietnam and other countries (1-3). Although UTIs have a lower mortality rate than other infections, they can lead to sepsis, thereby prolonging the duration of hospitalization and increasing treatment costs (4). Numerous studies have reported the severe consequences of infections caused by E. faecalis and P. aeruginosa, owing to their complex pathogenesis and the difficulty of selecting appropriate antibiotics for treatment (5,6).
Gram-positive E. faecalis is increasingly recognized as a major cause of hospital-acquired infections due to its intrinsic and acquired resistance mechanisms. According to evidence, its prevalence in UTIs ranges from 4.3% to 33.3% and from 2.7% to 6% in the north and south of Vietnam, respectively (7-12). High resistance rates have been reported, especially to tetracycline (81%–91.4%) and quinolones, such as levofloxacin (50–71.4%) and ciprofloxacin (35.7%). In contrast, resistance to linezolid remains low (3.6%), and no resistance has been detected to vancomycin, nitrofurantoin, fosfomycin, or daptomycin (7,8,10,11). Similar concerns have been raised by statistics from other countries; in Iran, the highest rate of resistance is to cotrimoxazole, vancomycin, and amikacin, while the lowest rate has been reported against nitrofurantoin (8.3%). Contrarily, in Germany, E. faecalis has led to 16.1% of UTI cases in male outpatients, with rising resistance to ciprofloxacin (13,14). These results highlight the necessity of continuous monitoring to direct the proper use of antibiotics and prevent the emergence of multidrug-resistant (MDR) strains.
Pseudomonas aeruginosa, a ubiquitous gram-negative organism, is associated with severe UTIs and exhibits high-level resistance to multiple antibiotic classes. Reports from both high-income and low-to-middle-income countries have documented increasing prevalence and resistance of these organisms in UTIs. In Vietnam, the prevalence of P. aeruginosa ranges from 7.9% to 15%, with resistance exceeding 50–70% for most antibiotics, including complete resistance to ciprofloxacin, norfloxacin, and ticarcillin/clavulanic acid. Moreover, resistance to cefepime and amikacin has been 36.7% and 22.7%, respectively (12,15-18). Studies from India and Iraq have reported similar findings (prevalence rates of 6.3% and 14%), with P. aeruginosa identified as one of the most drug-resistant pathogens. Although there was high susceptibility to meropenem, imipenem, amikacin, and tobramycin, and resistance to cefixime, cefotaxime, and ceftriaxone persisted, the majority of isolates were MDR (19,20). Recent isolates of P. aeruginosa in UTIs in Korea have demonstrated a high carbapenem resistance rate of 46.7% (21).
These bacterial species are often resistant to most antibiotics, including newly developed broad-spectrum agents (22,23). The emergence of MDR bacterial infection has become a global concern, imposing a significant burden on clinical practice (24). Accordingly, accurate and rapid identification of the etiology of UTIs and their antibiotic-resistance patterns can facilitate more targeted antibiotic selection, enhance treatment efficiency, reduce economic burden, and help limit the spread of antibiotic resistance (25). However, a limited number of studies have focused on evaluating E. faecalis and P. aeruginosa in central Vietnam. Therefore, this study aims to determine the prevalence of these bacteria in UTIs at Da Nang C Hospital, Vietnam, and to investigate the extent of their antibiotic resistance. Understanding the patterns of antibiotic resistance in P. aeruginosa and E. faecalis may help clinicians more effectively treat individuals who require antibiotics.
Materials and Methods
Sample Collection
Overall, 299 cultures of bacteria isolated from the urine samples of patients diagnosed with UTIs at Da Nang C Hospital were collected from January 2022 to December 2022. Midstream urine samples were collected for culture within 2 hours.
Quantitative Culture of Bacteria in Urine
According to the Health Ministry of Vietnam (26), there are several diagnostic criteria for UTIs. (a) If the bacterial count is lower than 10 colonies per plate ( < 10⁴ CFU/mL), the result is reported as “no significant bacterial growth detected.” (b) If the culture yields 10–100 colonies per plate (10⁴–10⁵ CFU/mL), further actions depend on clinical presentation. A repeat urine sample and quantitative culture are recommended for asymptomatic patients. On the other hand, identification and susceptibility testing should be performed in symptomatic patients with 1–2 bacterial species. In addition, the CFU count is reported with a recommendation for repeat urine collection and culture if symptoms are ambiguous and gram staining reveals low leukocyte and bacterial counts (c). Further, pathogen identification and antimicrobial susceptibility testing are required if bacterial growth exceeds 10⁵ CFU/mL with 1–2 dominant species (d). Finally, the sample is considered contaminated if cultures show polymicrobial growth ( > 2 species) in cases 2 and 3, and a properly collected urine specimen is required accordingly.
Bacterial Identification in Infected Urine Samples
Bacterial identification was performed using samples that reached clinically significant levels, as detailed in the previous part. Colony morphology was examined following cultivation on blood agar and MacConkey agar (selective for gram-negative bacteria; Merck, Germany) at 37 °C after 24 hours. Gram-positive bacteria collected in blood agar and gram-negative bacteria collected in MacConkey agar were identified using the Vitek 2 GP ID card and Vitek 2 GN ID card, respectively.
Antimicrobial Susceptibility Testing
Antibiotic susceptibility testing was performed using the disk-diffusion method (Kirby-Bauer test). Antibiotic discs were placed on Mueller-Hinton agar, and the inhibition zone diameter was measured according to the Clinical Laboratory Standards Institute protocol (2018). Penicillin G, ampicillin, rifampin, ciprofloxacin, levofloxacin, erythromycin, nitrofurantoin, linezolid, vancomycin, chloramphenicol, doxycycline, and tetracycline were antibiotics tested for E. faecalis. Ticarcillin/clavulanic acid, piperacillin/tazobactam, cefoperazone/sulbactam, ceftazidime, cefepime, imipenem, meropenem, amikacin, gentamicin, netilmicin, tobramycin, ciprofloxacin, levofloxacin, ofloxacin, clindamycin, and nitrofurantoin were tested for P. aeruginosa. The evaluation of MDR bacteria followed the criteria established by Magiorakos et al (22), defining MDR as resistance to at least one antibiotic in each of at least three different antimicrobial classes.
Statistical Analyses
The obtained data were transferred and managed using WHONET microbiology laboratory database software, while data analysis and data processing were performed using Excel.
Results
Distribution of Bacteria Causing Urinary Tract Infections in Hospital Departments
Bacteria that cause UTIs were detected in all departments of Da Nang C Hospital. These bacteria were most frequently isolated from the General Internal Medicine Department (27.1% of isolates), followed by surgery (23.7%), nephrology and urology (23.1%), intensive care unit (ICU) and stroke center (17.4%), and other departments (8.7%).
Prevalence of Enterococcus faecalis and Pseudomonas aeruginosa Causing Urinary Infections
Among the 299 bacterial strains causing UTIs in our study, Escherichia coli was the most prevalent (57.2%), followed by Klebsiella pneumoniae (17.7%), E. faecalis (10.0%), P. aeruginosa (8.7%), Proteus mirabilis (3.3%), and Acinetobacter baumannii (2.3%), while Staphylococcus aureus (0.7%) was the least common bacterium (27). Although E. coli and K. pneumoniae are the most common pathogens isolated in UTIs, E. faecalis and P. aeruginosa present more clinical challenges due to their complex resistance mechanisms and association with nosocomial infections. These characteristics make them important targets for detailed investigation in antimicrobial resistance surveillance and infection control strategies.
Table 1 presents the distribution of bacteria isolated from the departments. E. faecalis was more frequently isolated from the Department of Nephrology and Urology, as well as the ICU and the Stroke Center. P. aeruginosa was most commonly obtained from the Department of Surgery, followed by the Department of General Internal Medicine and Urology.
Table 1.
Distribution of E. faecalis and P. aeruginosa in Urine Samples Across Hospital Departments
|
Bacterium
|
General internal medicine
|
Endocrine urology
|
Surgery
|
Intensive care unit
and stroke center
|
Other departments
|
Total
|
|
Enterococcus faecalis
|
5 (16.7) |
8 (26.7) |
6 (20) |
8 (26.7) |
3 (10) |
30 (100) |
|
Pseudomonas aeruginosa
|
5 (19.2) |
5 (19.2) |
12 (46.2) |
2 (7.7) |
2 (7.7) |
26 (100) |
Data are expressed as Number (%).
Antibiotic Resistance of Enterococcus faecalis
Enterococcus faecalis exhibited high resistance rates (68%–88.9%) to ciprofloxacin, tetracycline, levofloxacin, and erythromycin (Figure 1). However, E. faecalis remained fully sensitive (100%) to linezolid. Importantly, 17 out of 30 E. faecalis isolates (56.7%) were classified as MDR.
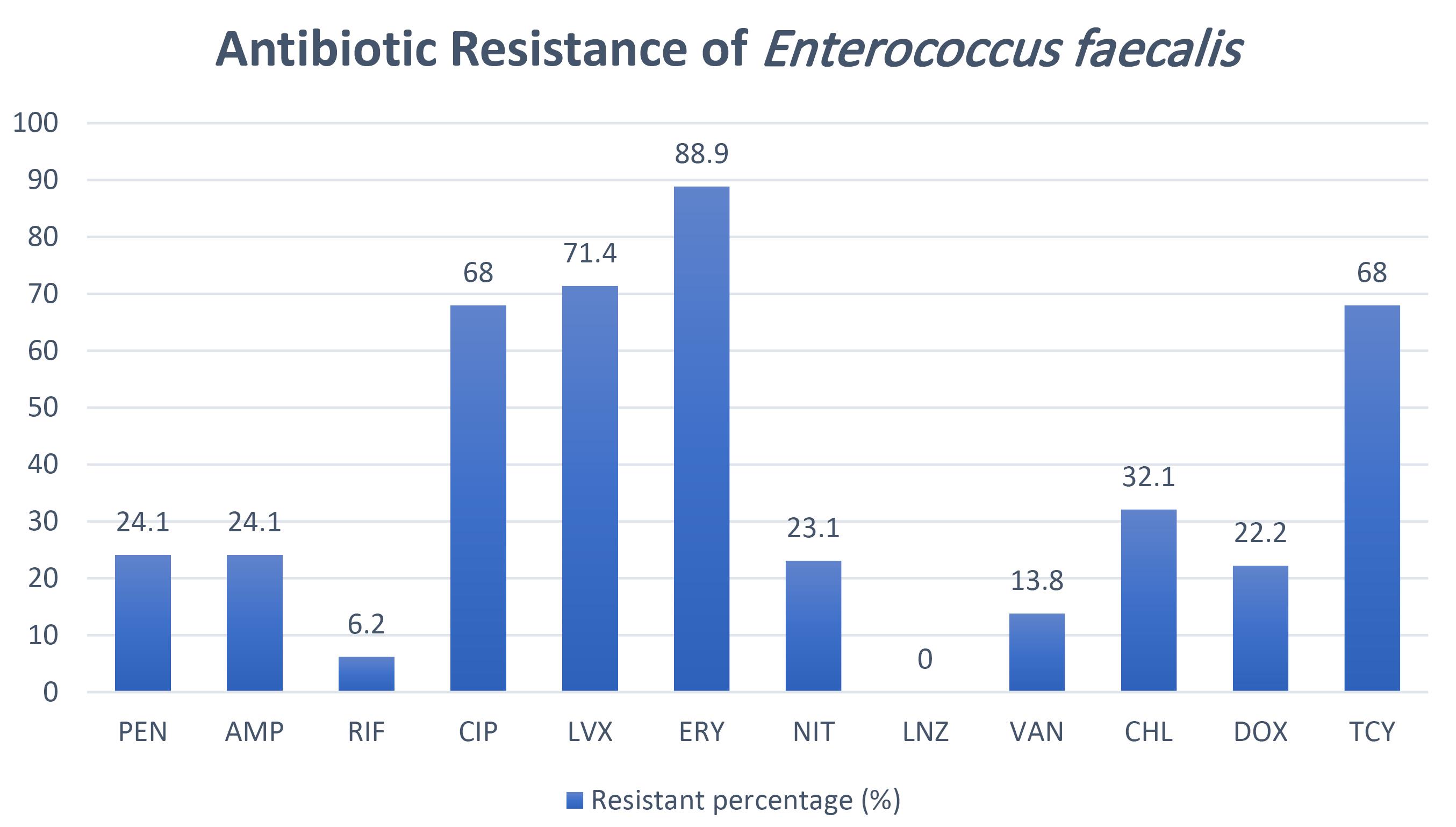
Figure 1.
Antibiotic Resistance of Enterococcus faecalis Isolates. Note. The number in each column indicates the percentage of isolates resistant to each antibiotic. PEN: Penicillin G; AMP: Ampicillin; RIF: Rifampin; CIP: Ciprofloxacin; LVX: Levofloxacin; ERY: Erythromycin; NIT: Nitrofurantoin; LNZ: Linezolid; VAN: Vancomycin; CHL: Chloramphenicol; DOX: Doxycycline; TCY: Tetracycline
.
Antibiotic Resistance of Enterococcus faecalis Isolates. Note. The number in each column indicates the percentage of isolates resistant to each antibiotic. PEN: Penicillin G; AMP: Ampicillin; RIF: Rifampin; CIP: Ciprofloxacin; LVX: Levofloxacin; ERY: Erythromycin; NIT: Nitrofurantoin; LNZ: Linezolid; VAN: Vancomycin; CHL: Chloramphenicol; DOX: Doxycycline; TCY: Tetracycline
Antibiotic Resistance of Pseudomonas aeruginosa
For Pseudomonas aeruginosa, resistance to tetracycline, levofloxacin, gentamicin, ciprofloxacin, tobramycin, ofloxacin, and nitrofurantoin was observed in 53.8–66.7% of the isolates (Figure 2). Notably, 9 out of 26 P. aeruginosa isolates (34.6%) were categorized as MDR.
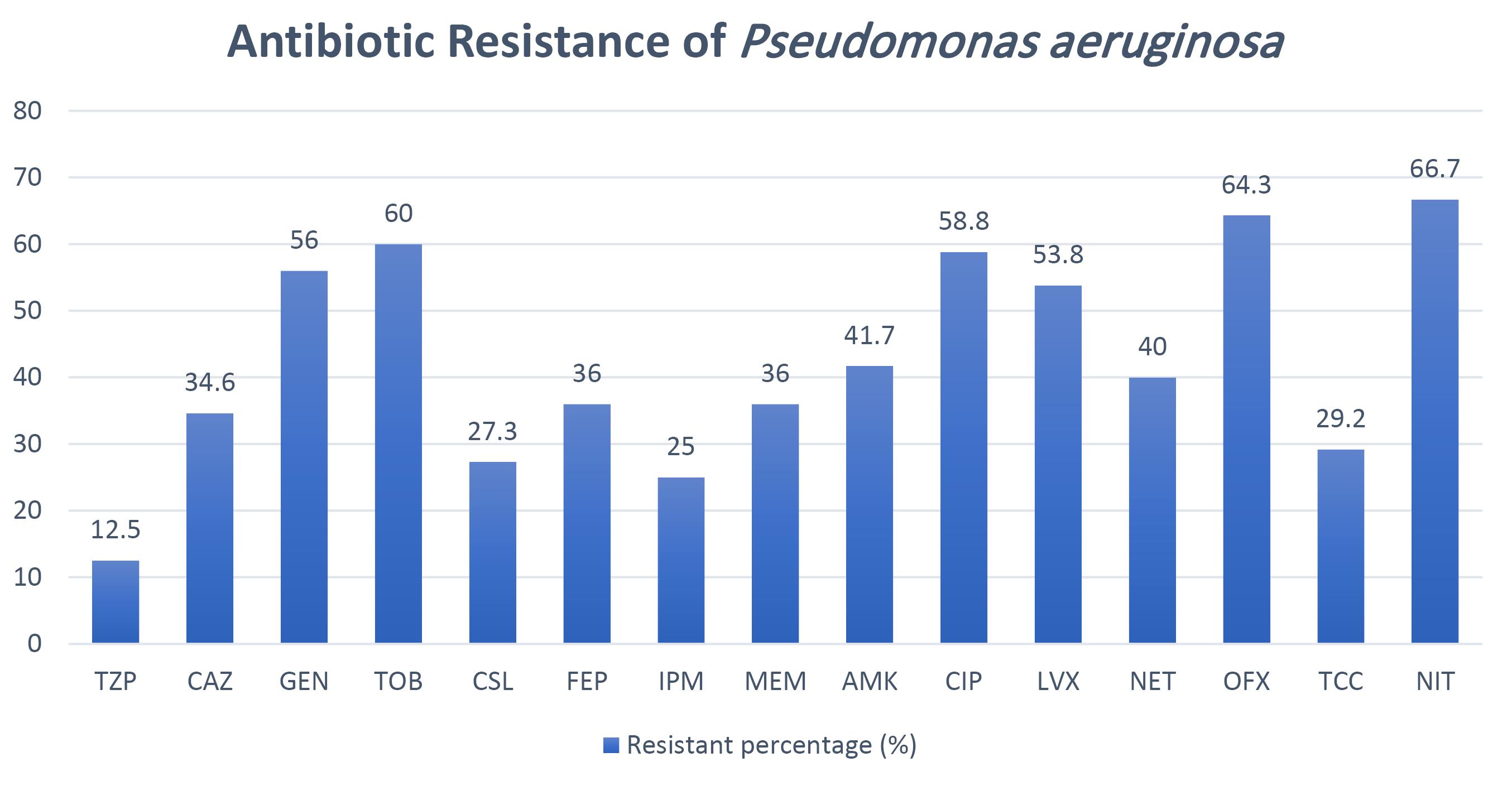
Figure 2.
Antibiotic Resistance of Pseudomonas aeruginosa Isolates. Note. The number in each column represents the percentage of isolates resistant to each antibiotic. TCC: Ticarcillin/clavulanic acid; TZP: Piperacillin/tazobactam; CSL: Cefoperazone/sulbactam; CAZ: Ceftazidime; FEP: Cefepime; IPM: Imipenem; MEM: Meropenem; AMK: Amikacin; GEN: Gentamicin; NET: Netilmicin; TOB: Tobramycin; CIP: Ciprofloxacin; LVX: Levofloxacin; OFX: Ofloxacin; CLI: Clindamycin; NIT: Nitrofurantoin
.
Antibiotic Resistance of Pseudomonas aeruginosa Isolates. Note. The number in each column represents the percentage of isolates resistant to each antibiotic. TCC: Ticarcillin/clavulanic acid; TZP: Piperacillin/tazobactam; CSL: Cefoperazone/sulbactam; CAZ: Ceftazidime; FEP: Cefepime; IPM: Imipenem; MEM: Meropenem; AMK: Amikacin; GEN: Gentamicin; NET: Netilmicin; TOB: Tobramycin; CIP: Ciprofloxacin; LVX: Levofloxacin; OFX: Ofloxacin; CLI: Clindamycin; NIT: Nitrofurantoin
Discussion
Prevalence of Enterococcus faecalis and Pseudomonas aeruginosa Causing Urinary Tract Infections at Da Nang C Hospital
Among 299 bacterial strains isolated from patients with UTIs across various departments, E. faecalis and P. aeruginosa were identified in 30 (10.03%) and 26 (8.69%) cases, respectively, which aligns with the results of a study performed in northern Vietnam (17), reporting an Enterococcus isolation rate of 10.57% but a higher P. aeruginosa rate (14.15%). In contrast, another study in Vietnam recorded lower isolation rates of E. faecalis (5%) and P. aeruginosa (8%) (28). In other countries, while P. aeruginosa may account for around 10–14% of UTIs in certain groups, E. faecalis prevalence appears to be more variable, occasionally lower than 10% in uncomplicated UTIs but higher in specific subgroups (29-33). While the reported prevalence varies, multiple studies confirm that E. faecalis and P. aeruginosa are significant causative agents of UTIs in hospitalized patients. The observed differences could be attributed to variations in study design, patient populations, clinical settings (community vs. hospital-acquired infections), and regional infection control practices.
In this study, E. faecalis and P. aeruginosa were isolated from patients in all departments. The rate of both bacterial species isolated from patients with UTIs at our ICU was higher than reported at hospitals in northern Vietnam (34). Higher detection rates for ICU patients likely reflect their severe clinical conditions and usually suppressed immune responses, thereby increasing susceptibility to illness (35-37). Urinary catheter placement in the surgery department is also a risk for hospital-acquired UTIs (38).
Antibiotic Resistance Among Enterococcus faecalis Isolates
Enterococcus faecalis is a gram-positive coccus, naturally resistant to several antibiotic classes, including cephalosporins and low-level aminoglycosides. The resistance of this bacterium to antibiotics significantly limits therapeutic options in clinical practice (39). In our study, E. faecalis isolates exhibited a high resistance rate (68%–88.9%) to ciprofloxacin, tetracycline, levofloxacin, and erythromycin. In contrast, the results revealed high susceptibility to linezolid, rifampin, and vancomycin, but moderate susceptibility to penicillin G, ampicillin, doxycycline, and chloramphenicol. Our results conform to those of the study performed by Nguyen and Binh at a hospital in northern Vietnam, where Enterococcus spp. demonstrated > 50% resistance to macrolides, tetracyclines, and fluoroquinolones (28). Similarly, a study in the north-central region of Vietnam reported resistance rates of 73.5% to ciprofloxacin and levofloxacin (17). Compared to a study conducted in northern Vietnam, our study showed higher resistance to fluoroquinolones (ciprofloxacin: 68%, levofloxacin: 71.4%), potentially due to differing local prescription practices for outpatients, including many elderly patients who often visit C Hospital for medical examinations. Internationally, a higher rate of resistance to vancomycin was reported in Iran (14). A recent systematic review has revealed a gradual increase in antibiotic resistance by E. faecalis worldwide, including resistance to linezolid (40). However, both vancomycin and linezolid remained efficacious in our study and in Vietnam as a whole (7,8,10,11), suggesting that differences in clinical antibiotic-prescribing practices between countries influence selective pressure and patterns of antibiotic resistance.
Antibiotic Resistance Among Pseudomonas aeruginosa Isolates
Pseudomonas aeruginosa displayed varying levels of resistance to all antibiotics tested in our study. High resistance rates ( > 50% of isolates) were observed against levofloxacin, gentamicin, ciprofloxacin, tobramycin, ofloxacin, and nitrofurantoin. These results are consistent with our previous findings (41). The resistance rates of P. aeruginosa to ceftazidime, cefepime, and piperacillin/tazobactam were higher than those reported in northern Vietnam (28). Contrarily, our study confirmed a lower frequency of resistance compared to a study in southern Vietnam (10), where resistance rates to ceftazidime, ciprofloxacin, cefepime, gentamicin, imipenem, meropenem, piperacillin/tazobactam, and nitrofurantoin exceeded 77%. While high susceptibility to meropenem, imipenem, amikacin, and tobramycin was observed in India and Iraq (19,20), our findings demonstrated relatively high resistance rates to these antibiotics (25%–60%), which is in line with the pattern reported in Korea (21). This discrepancy may be attributed to selective antibiotic pressure influenced by clinical prescribing practices, infection control, and microbial stewardship in individual countries. The aggressive use of empirical antibiotics in hospitals may drive the selection of more resistant P. aeruginosa strain.
Multidrug Resistance of Enterococcus faecalis and Pseudomonas aeruginosa
Out of 30 E. faecalis isolates, 17 (56.7%) were MDR (resistant to three or more antibiotic classes). The rate of MDR of E. faecalis in our study was higher than that in Romania (47.61%) (36) and lower than that in Egypt (74.6%) (42). Additionally, 34.6% of our P. aeruginosa isolates were identified as MDR. This MDR rate is lower than the frequencies of around 50% reported at a hospital in Pakistan in 2016 and 2019 (22,30), and much lower than the 77.2% reported in northern Vietnam from 2014 to 2021 (43). Overall, the frequency of MDR P. aeruginosa bacteria was lower compared to that reported in some national and international studies, implying that many isolates exhibited resistance to one or two drug classes, but were not concurrently resistant to ≥ 3 antibiotic classes as defined for MDR. The lower reported MDR rate may potentially be attributed to the preponderance of samples from non-critical patients in the surgery department rather than the ICU. Therefore, thorough profiling is necessary to precisely assess the clinical impact of resistance. In general, disparities in hospital-level infection control procedures, access to broad-spectrum antibiotics, study population, and antibiotic stewardship may all possibly contribute to the different MDR prevalence in the individual regions of both bacteria.
This study has provided updated data on the prevalence and antibiotic resistance of E. faecalis and P. aeruginosa in UTIs in Vietnam. Our results highlight multidrug resistance in E. faecalis, for which there is limited information in Vietnam. Our results further support the importance of regular surveillance and targeted antimicrobial stewardship to effectively manage infections caused by E. faecalis and P. aeruginosa. Nevertheless, this study was limited to a single hospital, which may not fully represent the prevalence and antibiotic resistance patterns of E. faecalis and P. aeruginosa in the region. Accordingly, it is recommended that further researchers perform multicenter studies with larger sample sizes to better represent regional trends. These should incorporate molecular techniques to identify resistance genes.
In this study, demographic information (including age and gender) was not collected, thereby limiting our ability to perform subgroup analyses. Nevertheless, our main goal was achieved, which was to concentrate on the microbiological traits and patterns of antibiotic resistance.
Conclusion
Our study highlights E. faecalis and P. aeruginosa as the significant causative agents of UTIs at Da Nang C Hospital, Central Vietnam. Both pathogens displayed high levels of antibiotic resistance, particularly to fluoroquinolones and β-lactam antibiotics. The detection of many MDR strains underscores the urgent need for continuous surveillance and effective antibiotic stewardship programs.
Acknowledgements
We would like to acknowledge Professor David Blair (Adjunct Professor at James Cook University, Australia) for his comments and manuscript editing.We would also like to thank Dr. Phan Thi Dieu Huyen, Head of the Department of Microbiology, Da Nang C Hospital, for supporting this work.
Competing Interests
The authors declare that they have no conflict of interests.
Data Availability Statement
The data used in this study were obtained from the WHONET surveillance system at Da Nang C Hospital, Da Nang, Vietnam. Due to patient confidentiality, ethical restrictions, and institutional regulations, the dataset cannot be shared publicly. Thus, access to the data requires permission from Da Nang C Hospital and the Ministry of Health of Vietnam.
Ethical Approval
The main ideas and framework of this study were authorized by the Ethics Committees of the Da Nang C Hospital and Da Nang University of Medical Technology and Pharmacy, Vietnam (54/CT-HĐĐĐ). All patients or their parents provided written informed consent before starting the study. The personal information of all patients was kept confidential.
Funding
This study was self-funded by the authors and received no external financial support from any funding organization.
References
- Que AT, Tran AD, Trang TH, Tran TNL, Bui NN, Lai CH. Epidemiology and antimicrobial resistance patterns of urinary tract infection: insights and strategies from a 5-year serial cross-sectional study in Vietnam. Ther Adv Infect Dis 2025; 12:20499361251315346. doi: 10.1177/20499361251315346 [Crossref] [ Google Scholar]
- Mancuso G, Midiri A, Gerace E, Marra M, Zummo S, Biondo C. Urinary tract infections: the current scenario and future prospects. Pathogens 2023; 12(4):623. doi: 10.3390/pathogens12040623 [Crossref] [ Google Scholar]
- Flores-Mireles AL, Walker JN, Caparon M, Hultgren SJ. Urinary tract infections: epidemiology, mechanisms of infection and treatment options. Nat Rev Microbiol 2015; 13(5):269-84. doi: 10.1038/nrmicro3432 [Crossref] [ Google Scholar]
- Foxman B. Urinary tract infection syndromes: occurrence, recurrence, bacteriology, risk factors, and disease burden. Infect Dis Clin North Am 2014; 28(1):1-13. doi: 10.1016/j.idc.2013.09.003 [Crossref] [ Google Scholar]
- Bongiovanni M, Barda B. Pseudomonas aeruginosa bloodstream infections in SARS-CoV-2 infected patients: a systematic review. J Clin Med 2023; 12(6):2252. doi: 10.3390/jcm12062252 [Crossref] [ Google Scholar]
- Scharloo F, Cogliati Dezza F, López-Hernández I, Martínez Pérez-Crespo PM, Goikoetxea Aguirre AJ, Pérez-Rodríguez MT. Clinical characteristics, predisposing factors and outcomes for Enterococcus faecalis versus Enterococcus faecium bloodstream infections: a prospective multicentre cohort study. Eur J Clin Microbiol Infect Dis 2024; 43(10):2011-22. doi: 10.1007/s10096-024-04917-5 [Crossref] [ Google Scholar]
- Nga NT, Hương ĐT, Sơn NV. Situation of antimicrobial resistance of common bacteria causing urinary tract infections at Hospital E. Vietnam Medical Journal 2025; 550(1):117-22. [ Google Scholar]
- Huy TQ, Uyên ĐT. The situation of bacterial strains causing urinary tract infections in inpatients at Military Hospital 175 in 2023. Vietnam Journal of Preventive Medicine 2024; 34(2):34-42. [ Google Scholar]
- Lâm BV, Thắng NĐ, Thuấn NĐ. Evaluation of treatment results of urinary tract infections caused by multi-drug resistant bacteria at Gia Dinh People’s Hospital. Vietnam Medical Journal 2023; 531(1):159-63. [ Google Scholar]
- Huy TQ, Lành TT, Trâm LN, Chương LV, Thảo TD. Urinary tract infection and antibiotic resistance at Kien Giang Provincial General Hospital in 2021. Vietnam Medical Journal 2023; 523(1):256-61. [ Google Scholar]
- Quế AT. Study on antibiotic resistance characteristics of gram-positive bacteria strains causing urinary tract infections isolated at Nghe An Friendship General Hospital. Vietnam Medical Journal 2022; 517(1):257-61. [ Google Scholar]
- Hòa NT, Linh BT, Dung NT, Thuỷ NT, Hà ĐT, Lâm ĐN. Catheter-associated urinary tract infections at the 108 Military Central Hospital: investigate the prevalence and antibiotic resistance of bacterial pathogens. Journal of 108 - Clinical Medicine and Pharmacy 2022; Medicine Conference 2022:98-103. [ Google Scholar]
- Salm J, Salm F, Arendarski P, Kramer TS. High frequency of Enterococcus faecalis detected in urinary tract infections in male outpatients - a retrospective, multicenter analysis, Germany 2015 to 2020. BMC Infect Dis 2023; 23(1):812. doi: 10.1186/s12879-023-08824-6 [Crossref] [ Google Scholar]
- Jafarzadeh Samani R, Tajbakhsh E, Momtaz H, Kabiri Samani M. Prevalence of virulence genes and antibiotic resistance pattern in Enterococcus faecalis isolated from urinary tract infection in Shahrekord, Iran. Rep Biochem Mol Biol 2021; 10(1):50-9. doi: 10.52547/rbmb.10.1.50 [Crossref] [ Google Scholar]
- Chi LT, Vân NT. Determination of antimicrobial susceptibility of bacteria isolated from patients with urinary tract infections at Hue University of Medicine and Pharmacy Hospital. Hue Journal of Medicine and Pharmacy 2024; 14(5):144-52. [ Google Scholar]
- Lành PT, Hồ NN, Khôi NN. Investigating on antibiotic use in the treatment of urinary tract infections at Thong Nhat General Dong Nai Hospital. Vietnam Medical Journal 2023; 523(2):59-64. [ Google Scholar]
- Trâm QA, Hoa LN, Đào TA. Study on antibiotic resistance of bacterial strains causing urinary tract infections isolated at Nghe An General Hospital. J Clin Med 2021; 517(1):257-61. [ Google Scholar]
- Thức NT, Mạnh NĐ. Research antibiotic resistance and rate of bacteria cause urinary tract infections in patients placed urinary catheter. Journal of 108 - Clinical Medicine and Pharmacy 2018; 13(6):25-30. [ Google Scholar]
- Salman HA, Alhameedawi AK, Alsallameh SM, Muhamad G, Taha Z. Prevalence of multi-antibiotic resistant bacteria isolated from children with urinary tract infection from Baghdad, Iraq. Microbiol Biotechnol Lett 2022; 50(1):147-56. doi: 10.48022/mbl.2110.10011 [Crossref] [ Google Scholar]
- Bhargava K, Nath G, Bhargava A, Kumari R, Aseri GK, Jain N. Bacterial profile and antibiotic susceptibility pattern of uropathogens causing urinary tract infection in the eastern part of Northern India. Front Microbiol 2022; 13:965053. doi: 10.3389/fmicb.2022.965053 [Crossref] [ Google Scholar]
- Park Y, Koo SH. Epidemiology, molecular characteristics, and virulence factors of carbapenem-resistant Pseudomonas aeruginosa isolated from patients with urinary tract infections. Infect Drug Resist 2022; 15:141-51. doi: 10.2147/idr.S346313 [Crossref] [ Google Scholar]
- Magiorakos AP, Srinivasan A, Carey RB, Carmeli Y, Falagas ME, Giske CG. Multidrug-resistant, extensively drug-resistant and pandrug-resistant bacteria: an international expert proposal for interim standard definitions for acquired resistance. Clin Microbiol Infect 2012; 18(3):268-81. doi: 10.1111/j.1469-0691.2011.03570.x [Crossref] [ Google Scholar]
- Vo TH, Bui QH, Nguyen HH, Pham HT. Antimicrobial resistance patterns of Pseudomonas aeruginosa in a Vietnamese Tertiary Care Hospital. Int J Trop Dis 2022; 5(1):58. doi: 10.23937/2643-461x/1710058 [Crossref] [ Google Scholar]
- Shrivastava SR, Shrivastava PS, Ramasamy J. World Health Organization releases global priority list of antibiotic-resistant bacteria to guide research, discovery, and development of new antibiotics. J Med Soc 2018; 32(1):76-7. doi: 10.4103/jms.jms_25_17 [Crossref] [ Google Scholar]
- Tängdén T, Giske CG. Global dissemination of extensively drug-resistant carbapenemase-producing Enterobacteriaceae: clinical perspectives on detection, treatment and infection control. J Intern Med 2015; 277(5):501-12. doi: 10.1111/joim.12342 [Crossref] [ Google Scholar]
- Ministry of Health. Clinical Microbiology Laboratory Techniques Ministry of Health of Vietnam. Ministry of Health; 2017.
- Suong TT, Trinh NT. Survey the antibiotic resistance of Escherichia coli and Klebsiella pneumoniae causing urinary tract infections at Da Nang C Hospital. Vietnam Journal of Community Medicine 2023; 64(9):90-7. [ Google Scholar]
- Nguyen TN, Binh LT. Characteristics of patients with complex urinary tract infection in Thai Nguyen Central Hosiptal. Vietnam Medical Journal 2022; 508(2):1-6. [ Google Scholar]
- Johnson B, Stephen BM, Joseph N, Asiphas O, Musa K, Taseera K. Prevalence and bacteriology of culture-positive urinary tract infection among pregnant women with suspected urinary tract infection at Mbarara Regional Referral Hospital, South-Western Uganda. BMC Pregnancy Childbirth 2021; 21(1):159. doi: 10.1186/s12884-021-03641-8 [Crossref] [ Google Scholar]
- Reynolds D, Kollef M. The epidemiology and pathogenesis and treatment of Pseudomonas aeruginosa infections: an update. Drugs 2021; 81(18):2117-31. doi: 10.1007/s40265-021-01635-6 [Crossref] [ Google Scholar]
- Bayyiğit A, Erdem MG, Ünlü Ö, Demirci M. Urinary Tract Infections Caused by Pseudomonas aeruginosa: An 11-Year Retrospective Analysis on Antimicrobial Resistance. European Archives of Medical Research 2023; 39:189-95. doi: 10.4274/eamr.galenos.2023.16046 [Crossref] [ Google Scholar]
- Codelia-Anjum A, Lerner LB, Elterman D, Zorn KC, Bhojani N, Chughtai B. Enterococcal urinary tract infections: a review of the pathogenicity, epidemiology, and treatment. Antibiotics (Basel) 2023; 12(4):778. doi: 10.3390/antibiotics12040778 [Crossref] [ Google Scholar]
- Garout W. Prevalence and risk factors of urinary tract infection among children with bronchiolitis. Pediatr Neonatol 2024; 65(4):348-53. doi: 10.1016/j.pedneo.2023.08.009 [Crossref] [ Google Scholar]
- Thu NT, Duy ĐV, Huyền DT, Phượng TT, Thuận HT, Huân LX. Survey on the characteristics of urinary tract infections in intensive care unit at 108 Military Central Hospital. Journal of 108 - Clinical Medicine and Pharmacy 2022; 17:222-7. [ Google Scholar]
- Schärer V, Meier MT, Schuepbach RA, Zinkernagel AS, Boumasmoud M, Chakrakodi B. An intensive care unit outbreak with multi-drug-resistant Pseudomonas aeruginosa - spotlight on sinks. J Hosp Infect 2023; 139:161-7. doi: 10.1016/j.jhin.2023.06.013 [Crossref] [ Google Scholar]
- Golli AL, Cristea OM, Zlatian O, Glodeanu AD, Balasoiu AT, Ionescu M. Prevalence of multidrug-resistant pathogens causing bloodstream infections in an intensive care unit. Infect Drug Resist 2022; 15:5981-92. doi: 10.2147/idr.S383285 [Crossref] [ Google Scholar]
- Gill JS, Arora S, Khanna SP, Kumar KH. Prevalence of multidrug-resistant, extensively drug-resistant, and pandrug-resistant Pseudomonas aeruginosa from a tertiary level intensive care unit. J Glob Infect Dis 2016; 8(4):155-9. doi: 10.4103/0974-777x.192962 [Crossref] [ Google Scholar]
- Cattaneo C, Rieg S, Schwarzer G, Müller MC, Blümel B, Kern WV. Enterococcus faecalis bloodstream infection: does infectious disease specialist consultation make a difference?. Infection 2021; 49(6):1289-97. doi: 10.1007/s15010-021-01717-3 [Crossref] [ Google Scholar]
- Geraldes C, Tavares L, Gil S, Oliveira M. Enterococcus virulence and resistant traits associated with its permanence in the hospital environment. Antibiotics (Basel) 2022; 11(7):857. doi: 10.3390/antibiotics11070857 [Crossref] [ Google Scholar]
- Guan L, Beig M, Wang L, Navidifar T, Moradi S, Motallebi Tabaei F. Global status of antimicrobial resistance in clinical Enterococcus faecalis isolates: systematic review and meta-analysis. Ann Clin Microbiol Antimicrob 2024; 23(1):80. doi: 10.1186/s12941-024-00728-w [Crossref] [ Google Scholar]
- Trinh NT, Phương PT, Hòa HT, Hoàng NH. Pathogenic characteristics and antibiotic resistance of Pseudomonas aeruginosa at Da Nang C Hospital. Can Tho Journal of Medicine and Pharmacy. 2023(58):159-66.
- Said HS, Abdelmegeed ES. Emergence of multidrug resistance and extensive drug resistance among enterococcal clinical isolates in Egypt. Infect Drug Resist 2019; 12:1113-25. doi: 10.2147/idr.S189341 [Crossref] [ Google Scholar]
- Le HHL, Thuc LC, Ta TB, Tran TV, Hung DV, Kien HT. Prevailing antibiotic resistance patterns in hospitalized patients with urinary tract infections in a Vietnamese Teaching Hospital (2014-2021). Infect Drug Resist 2025; 18:613-23. doi: 10.2147/idr.S499804 [Crossref] [ Google Scholar]