Avicenna Journal of Clinical Microbiology and Infection. 12(4):220-230.
doi: 10.34172/ajcmi.3627
Review Article
Epidemiology and Etiology of Bacterial Meningitis in Iran: A Systematic Review and Meta-analysis
Mohammad Hossein Ekvan Conceptualization, Data curation, Investigation, Methodology, Validation, Visualization, Writing – original draft, 1 
Omid Raiesi Conceptualization, Funding acquisition, Methodology, Project administration, Resources, Supervision, Validation, Visualization, Writing – review & editing, 2, *
Muhammad Ibrahim Getso Writing – review & editing, 3
Masoume Karimi Formal analysis, Software, Validation, 4
Somayeh Mohamadi Data curation, 1
Amir Hossein Ahmadi Investigation, 1
Maryam Kord Data curation, 1
Sara Tabar Data curation, 1
Author information:
1Student Research Committee, Ilam University of Medical Sciences, Ilam, Iran
2Department of Parasitology, School of Allied Medical Sciences, Ilam University of Medical Sciences, Ilam, Iran
3Department of Medical Microbiology and Parasitology, College of Health Sciences, Bayero University, PMB, 3011, Kano, Nigeria
4Department of Epidemiology, School of Public Health, Ilam University of Medical Sciences, Ilam, Iran
Abstract
Background: Meningitis is a life-threatening disease that can manifest as acute, subacute, or chronic. This disease is characterized by various symptoms such as fever, nausea, and stiff neck. It can be caused by infectious (bacteria, viruses, fungi, and parasites) and non-infectious (drugs, neoplasms, and systemic diseases) agents. Bacterial meningitis, the deadliest type of meningitis, was the focus of this systematic review and meta-analysis, which aimed to examine the epidemiology and etiology of bacterial meningitis in Iran.
Methods: PubMed (Medline), Scopus, Web of Science, and ProQuest were searched for English articles and the Scientific Information Database and Magiran for Persian articles up to January 25, 2024. A total of 2240 articles were screened, and 58 articles were selected. Then, 51 studies were included in the epidemiological analysis and 48 in the etiological analysis.
Results: The pooled hospital-based prevalence of meningitis in Iran was 16.48%. Streptococcus pneumoniae was responsible for 27.89% of meningitis cases in Iran and was the main cause of bacterial meningitis. Other common bacteria included Haemophilus influenzae (15.96%), Staphylococcus epidermidis (15.88%), and Klebsiella pneumoniae (15.56%). Fever was observed in 89.37% of patients, while nausea, neck stiffness, vomiting, and headache were also common manifestations, affecting approximately half of the patients.
Conclusion: These findings highlight the importance of vaccination, especially against pneumococcus, and improved diagnostic practices. The results also underscore the need for stronger surveillance systems and expanded population coverage to enhance public health interventions and reduce the burden of bacterial meningitis in Iran.
Keywords: Bacterial, Meningitis, Systematic review, Mata-analysis, Iran
Copyright and License Information
© 2025 The Author(s); Published by Hamadan University of Medical Sciences.
This is an open-access article distributed under the terms of the Creative Commons Attribution License (
https://creativecommons.org/licenses/by/4.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Please cite this article as follows: Ekvan MH, Raiesi O, Getso MI, Karimi M, Mohamadi S, Ahmadi AH, et al. Epidemiology and etiology of bacterial meningitis in Iran: a systematic review and meta-analysis. Avicenna J Clin Microbiol Infect. 2025;12(4):220-230. doi:10.34172/ajcmi.3627
Introduction
Meningitis is the inflammation of any of the three meningeal layers surrounding the brain or spinal cord, accompanied by pleocytosis in the cerebrospinal fluid (CSF). Meningitis is classified as acute ( ≤ 5 days), subacute ( ≤ 5 days), and chronic ( ≥ 4 weeks) (1-3). This condition is typically accompanied by fever, nausea, stiff neck, and headache (4). Other clinical manifestations may include changes in mental status, altered level of consciousness, seizures, photophobia, and skin rashes (5,6). CSF analysis is required for a definitive diagnosis (7-9). Meningitis can be caused by infectious agents (bacteria, viruses, fungi, and protozoa) or non-infectious causes (drugs, neoplasms, and some systemic diseases). If bacteria are found in CSF, it is called bacterial meningitis; otherwise, it is called aseptic meningitis (10,11). In 3approximately 0 to 65% of cases, the definitive cause of aseptic meningitis is unidentified (12).
According to the Centers for Disease Control and Prevention (CDC), viral and then bacterial infections are the most common causes of meningitis, with bacterial meningitis being the most dangerous type. If untreated, bacterial meningitis can be fatal in up to 50% of cases. Even with prompt treatment, 8 to 15% of patients may die within two days of symptom onset (13). The etiology of bacterial meningitis varies depending on age and regional microbial flora. A review study conducted in 2015 examined articles related to acute meningitis in Iran and revealed that Streptococcus pneumoniae, Haemophilus influenzae type b, coagulase-negative Staphylococcus aureus, and Neisseria meningitidis were the most common causative agents (14). Another study identified S. pneumoniae and N. meningitidis as the most common bacteria causing the disease (15). This systematic review and meta-analysis aimed to achieve two main objectives: (1) to estimate the pooled prevalence of bacterial meningitis in Iran, and (2) to determine the most common bacterial species causing meningitis in Iran. In addition, the review will examine clinical manifestations presented in the included articles.
Methods
A systematic search was conducted to identify articles related to patients with bacterial meningitis in Iran. The protocol for this study was registered in Prospero (Registration number: CRD42024507783) on February 17, 2024. Relevant articles were identified using keywords such as “meningitis”, “bacterial”, and “Iran” along with their synonyms, as MeSH terms, in the title, abstract, and keywords. The international databases PubMed (Medline), Scopus, Web of Science, and ProQuest were searched until January 25, 2024. The search strategy for PubMed was as follows: ((((Meningit*[MeSH Terms]) OR (Pachymeningit*[MeSH Terms])) OR ((Meningit*[tiab]) OR (Pachymeningit*[tiab]))) AND (((Bacteria*[MeSH Terms]) OR (Eubacteria*[MeSH Terms])) OR ((Bacteria*[tiab]) OR (Eubacteria*[tiab])))) AND (Iran*). Additionally, local databases such as the Scientific Information Database and the Magiran database were searched for Persian articles using the same search strategy and similar Persian keywords. Then, Google Scholar and the latest relevant review article (14) were searched to maximize the number of relevant articles.
Inclusion and Exclusion Criteria
All English and Persian articles related to the epidemiology and etiology of bacterial meningitis in Iran were included in the study, with no time limit applied. Articles were excluded if: (a) They were letters to the editor, reviews, intervention studies, cohort studies, or case-control studies; (b) They did not use a standard CSF test for diagnosis; (c) They involved patients with abnormal immune systems (e.g., patients with HIV, agranulocytosis, and the like); or (d) Studies that focused on the identification of one specific bacterial species.
Screening Process
All articles from the search results were entered into EndNote 21 software. After removing duplicate articles, two independent researchers screened the articles in three stages based on title, abstract, and full text. Any disagreements in the final selection of articles were resolved through consultation between two researchers, with the opinion of a third researcher sought if necessary.
Data Extraction
Two independent researchers performed data extraction. The extracted data included title, first author, year of publication, study location, study period, total number of samples, number of confirmed cases, type of meningitis, and the etiologic agent of meningitis. Other data extracted from the articles included clinical manifestations and/or drug resistance. These data were only analyzed if reported in at least 10% of the articles.
Quality Assessment
For quality assessment, two independent researchers used a modified version of the Newcastle-Ottawa Scale, specifically adapted for cross-sectional studies, as applied in a previous study (16). This version was originally adapted from the Newcastle-Ottawa Scale for cohort studies to suit cross-sectional designs, and it included seven questions across three domains: selection, confounders, and exposure. The domains covered key elements such as sampling strategy, response rate, exposure assessment, and statistical reporting. The total score ranged from 0 to 10. Studies were classified based on their total score as follows: very good (9–10 points), good (7–8 points), satisfactory (5–6 points), and unsatisfactory (0–4 points). Articles categorized as “unsatisfactory” were excluded from the study. Any disagreements between reviewers were resolved by a third independent researcher.
Meta-Analysis
Data analysis was conducted using Stata 11 software. The Metaprop command was used to calculate the pooled prevalence along with a 95% confidence interval (CI), results of which were presented in a forest plot. To assess the heterogeneity of studies, the Chi-square test and the I2 index were used. Based on the Hygienist classification, studies with an I2 index heterogeneity rate of more than 75% were considered in the very high heterogeneity category, 50–75% in the high heterogeneity category, 25–50% in the moderate heterogeneity category, and less than 25% in the low heterogeneity category. If the I2 index was higher than 50%, a random-effects model using the DerSimonian and Laird method was used to estimate the pooled prevalence. Additionally, meta-regression was used to investigate the sources of heterogeneity in the results. The “metabias” command was used to check for publication bias, based on the results of the Egger test. In the case of observed bias, prevalence rates were corrected using the “metatrim” command with the “trim-and-fill” method. A significance level of 0.05 was set for all analyses.
Results
A total of 2240 articles were identified through a search of six databases, including the most recent relevant study (14), as depicted in Figure 1. After removing 543 duplicate articles, we screened 1697 articles. We excluded 1,313 articles in the first stage and 277 articles in the second stage, and reviewed the full text of 107 articles. Finally, we excluded 49 additional articles and found 58 articles eligible for inclusion in this review, including 10 articles in Persian and 48 articles in English. Of these, 52 articles were included in the epidemiological analysis, while 48 articles were included in the etiological analysis (Figure 2). The studies covered 17 different cities. Most of the articles were from Tehran (n = 26), all of which were hospital-based studies. All diagnoses were confirmed by bacterial culture from CSF. If diagnosed using other methods, only samples with positive bacterial culture of CSF were included in this review. The primary objective of the study was to conduct categorical analyses based on acute, subacute, and chronic types. However, this was limited by the small number of studies on subacute and chronic types, as well as the lack of specification regarding meningitis types in many articles, making it impossible to separate these cases. Thus, all study data were examined cumulatively.
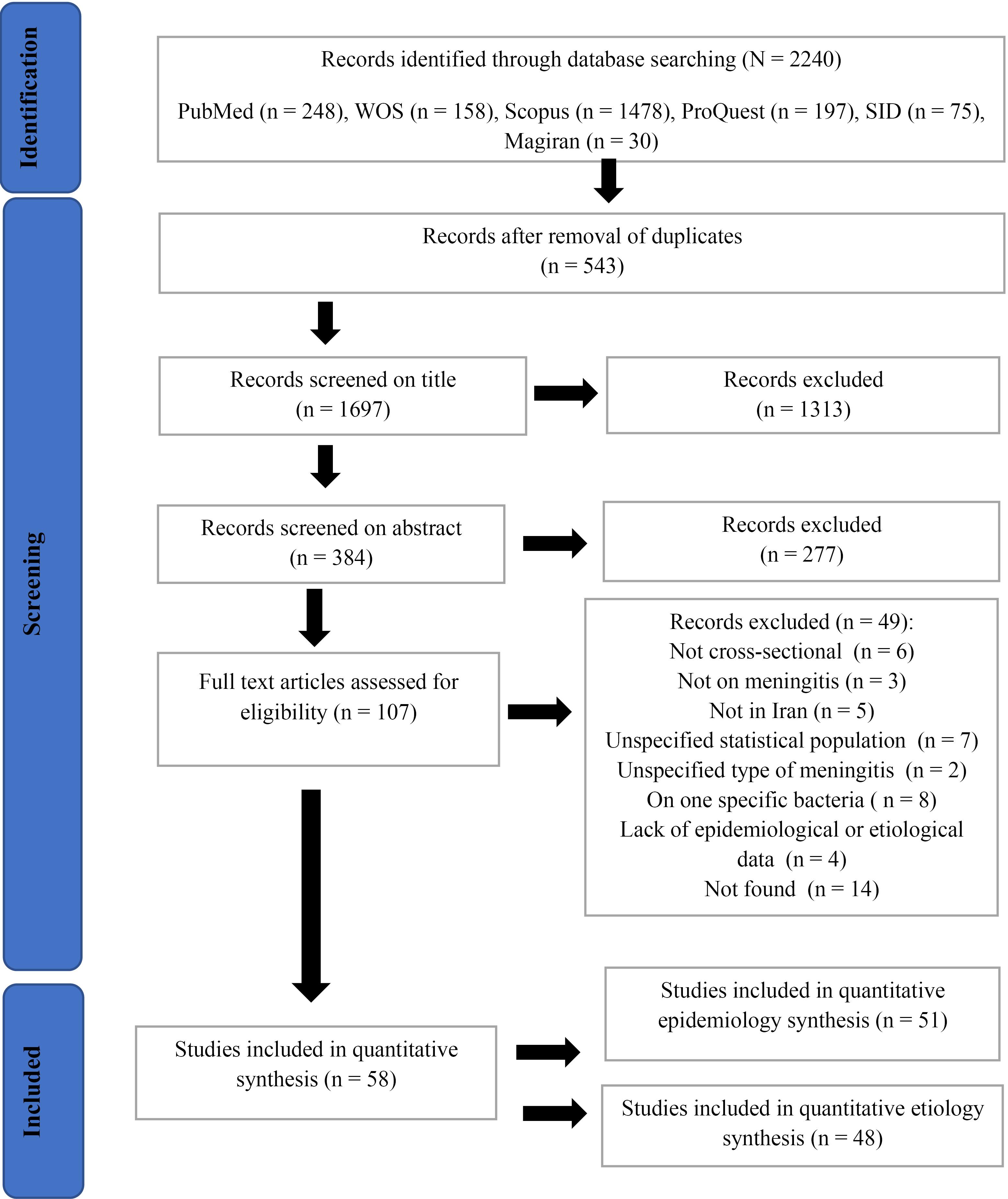
Figure 1.
Search Flow Diagram and Article Screening
.
Search Flow Diagram and Article Screening
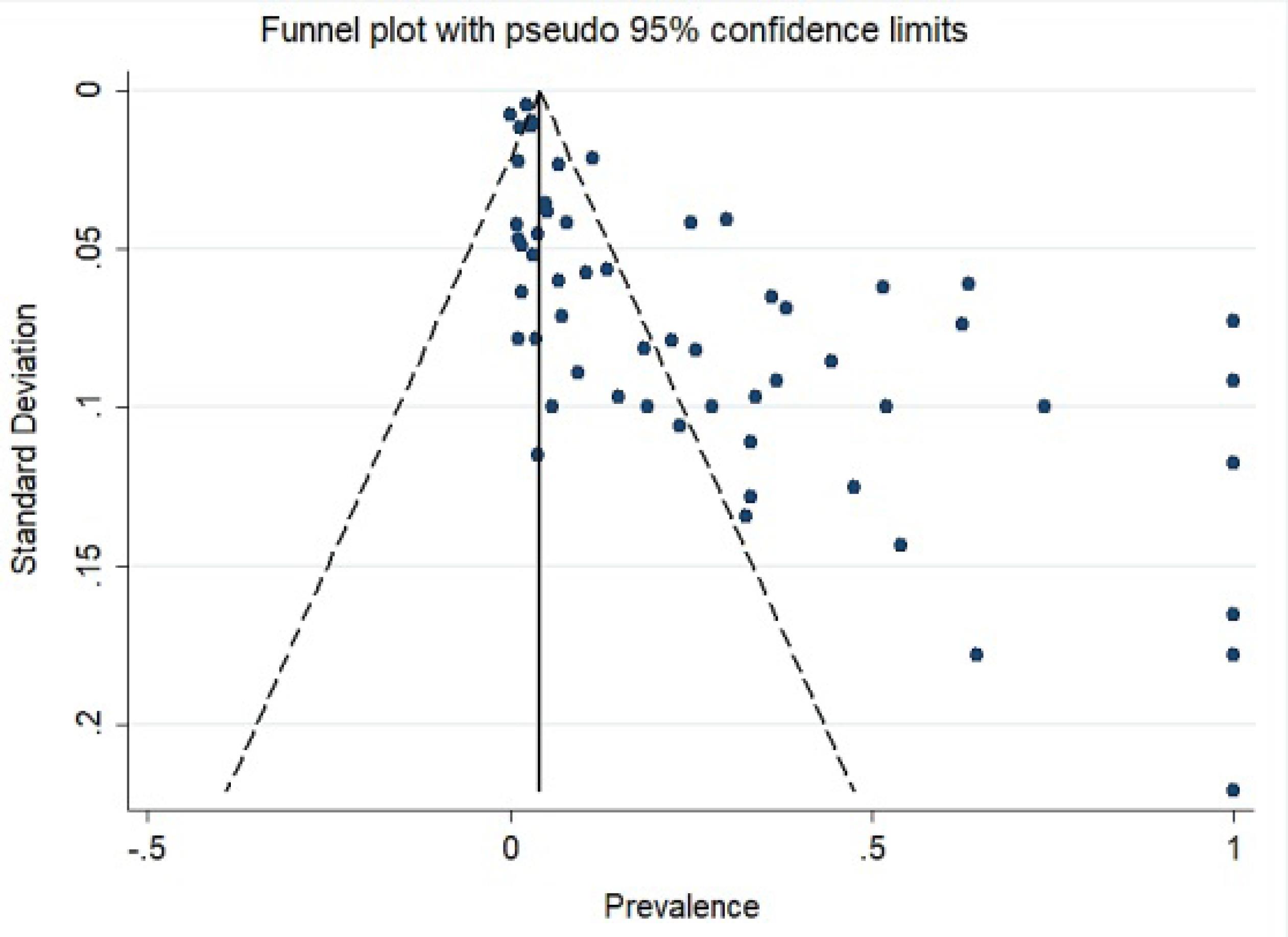
Figure 2.
Funnel Chart for Imported Articles
.
Funnel Chart for Imported Articles
Epidemiology of Bacterial Meningitis
In this section, we included 51 articles collected from 17 different cities (Table 1). A total of 107 766 cases were examined, of which 4062 were diagnosed with bacterial meningitis. As all studies were conducted in hospital settings, the resulting epidemiological data reflect a hospital-based perspective. Therefore, we were unable to estimate the broader community epidemiology. The epidemiology of bacterial meningitis in Iranian hospitals was 16.48% (95% CI: 13.70 – 19.46; I2: 99.16%), as illustrated in Figure 3. Patients ranged from infants to adults over 65 years, with approximately half being under 6 years old and 90% under 18 years. The prevalence in different studies ranged from 74% (17) to 0.14% (18). This epidemiological overview covered 25 years. The oldest article was published in 1998 (19), while the most recent studies appeared in 2022 (20-23). Most studies (n = 33) were published within the last decade (2013-2023).
Table 1.
Characteristics of Articles Reviewed on the Prevalence of Meningitis in Iran
|
First Author
|
Sampling Area
|
Published Time
|
Study Sample
|
Diagnosis With Meningitis
|
Prevalence of Meningitis (%)
|
95% CI
|
| Yousefi Mashouf et al (24) |
Hamedan |
2013 |
582 |
46 |
7.9 |
5.84 - 10.40 |
| Ghadimi Moghaddam et al (25) |
Yasuj |
2019 |
106 |
36 |
33.96 |
25.04 - 43.80 |
| Samiee-Rad and Karimfar (26) |
Ghazvin |
2012 |
567 |
6 |
1.06 |
0.39 - 2.29 |
| Amid et al (19) |
Tehran |
1998 |
609 |
182 |
29.89 |
26.27 - 33.69 |
| Ehsanipour et al (27) |
Tehran |
2005 |
245 |
4 |
1.63 |
0.45 - 4.13 |
| Ataei et al (28) |
Tehran |
2005 |
100 |
28 |
28 |
19.48 - 37.87 |
| Yousefi Mashouf et al (29) |
Hamedan |
2006 |
582 |
146 |
25.09 |
21.61 - 28.81 |
| Taheri Kalani et al (30) |
Tehran |
2006 |
300 |
32 |
10.67 |
7.41 - 14.72 |
| Haghi-Ashtiani et al (31) |
Tehran |
2008 |
1800 |
121 |
6.72 |
5.61 - 7.98 |
| Bahador et al (32) |
Kerman |
2009 |
126 |
12 |
9.52 |
5.02 - 16.05 |
| Alavi et al (33) |
Ahvaz |
2010 |
312 |
42 |
13.46 |
9.88 - 17.76 |
| Hatami et al (34) |
Tehran |
2010 |
793 |
39 |
4.92 |
3.52 - 6.66 |
| Bayat Makoo et al (35) |
Tabriz |
2010 |
100 |
19 |
19 |
11.84 - 28.07 |
| Qurbanalizadegan et al (36) |
Tehran |
2010 |
161 |
36 |
22.36 |
16.18 - 29.59 |
| Sarookhani et al (17) |
Ghazvin |
2010 |
100 |
74 |
74 |
64.27 - 82.26 |
| Ataee et al (37) |
Tehran |
2011 |
270 |
171 |
63.33 |
57.28 - 69.09 |
| Ghotaslou et al (38) |
Tabriz |
2012 |
277 |
19 |
6.86 |
4.18 - 10.50 |
| Hamedi et al (39) |
Mashhad |
2012 |
81 |
27 |
33.33 |
23.24 - 44.68 |
| Hojjati Bonab et al (40) |
Tabriz |
2012 |
106 |
16 |
15.09 |
8.88 - 23.35 |
| Rezaeizadeh et al (41) |
Tehran |
2012 |
11269 |
329 |
2.92 |
2.62 - 3.25 |
| Mahmoudi et al (42) |
Tehran |
2013 |
31 |
20 |
64.52 |
45.37 - 80.77 |
| Rezaei et al (43) |
Tehran |
2013 |
55 |
18 |
32.73 |
20.68 - 46.71 |
| Abdinia et al (44) |
Tabriz |
2014 |
7112 |
107 |
1.5 |
1.23 - 1.82 |
| Attarpour-Yazdi et al (45) |
Tehran |
2014 |
182 |
114 |
62.64 |
55.17 - 69.68 |
| Babamahmoodi et al (46) |
Mazandaran |
2014 |
16532 |
23 |
0.14 |
0.09 - 0.21 |
| Heydarian et al (18) |
Mashhad |
2014 |
453 |
5 |
1.1 |
0.36 - 2.56 |
| Tavasoli et al (47) |
Tehran |
2014 |
422 |
7 |
1.66 |
0.67 - 3.39 |
| Bagheri-Nesami et al (48) |
Mazandaran |
2015 |
137 |
61 |
44.53 |
36.04 - 53.25 |
| Moayedi et al (49) |
Bandar Abbas |
2015 |
100 |
6 |
6 |
2.23 - 12.60 |
| Motamedifar et al (50) |
Shiraz |
2015 |
2229 |
255 |
11.44 |
10.15 - 12.83 |
| Shirani et al (51) |
Esfahan |
2015 |
2229 |
6 |
3.7 |
1.37 - 7.89 |
| Amin et al (52) |
Ahvaz |
2016 |
196 |
14 |
7.14 |
3.96 - 11.69 |
| Farahani et al (53) |
Arak |
2016 |
150 |
28 |
18.67 |
12.78 - 25.84 |
| Jesri et al (54) |
Iran |
2016 |
8411 |
250 |
2.97 |
2.62 - 3.36 |
| Moafi et al (55) |
Ghazvin |
2016 |
680 |
35 |
5.15 |
3.61 - 7.09 |
| Vakili et al (56) |
Yazd |
2016 |
261 |
135 |
51.72 |
39.17 - 68.63 |
| Mofidi et al (57) |
Tehran |
2017 |
48 |
26 |
54.17 |
39.17 - 68.63 |
| Sanaei Dashti et al (58) |
Tehran |
2017 |
370 |
12 |
3.24 |
1.69 - 5.60 |
| Berangi et al (59) |
Hamedan |
2019 |
48006 |
1135 |
2.36 |
2.23 - 2.50 |
| Hadi et al (60) |
Shiraz |
2019 |
89 |
21 |
23.6 |
15.24 - 33.78 |
| Pormohammad et al (61) |
Tehran |
2019 |
119 |
44 |
36.97 |
28.31 - 46.31 |
| Boskabadi et al (62) |
Mashhad |
2020 |
234 |
85 |
36.32 |
30.16 - 42.84 |
| Kashaki et al (63) |
Tehran |
2020 |
75 |
3 |
4 |
0.38 - 11.25 |
| Saboute et al (64) |
Tehran |
2020 |
163 |
2 |
1.23 |
0.15 - 4.36 |
| Hemmati et al (65) |
Ghazvin |
2021 |
212 |
81 |
38.21 |
31.64 - 45.11 |
| Mirjalili et al (66) |
Tehran /Karaj |
2021 |
148 |
38 |
25.68 |
18.85 - 33.50 |
| Zeighami et al (67) |
Zanjan |
2021 |
100 |
52 |
52 |
41.78 - 62.10 |
| Bineshfar et al (20) |
Kerman |
2022 |
2050 |
25 |
1.22 |
0.79 - 1.80 |
| Farokhnia et al (21) |
Kerman |
2022 |
60 |
20 |
33.33 |
21.69 - 46.69 |
| Pouladfar et al (22) |
Shiraz |
2022 |
492 |
19 |
3.86 |
2.34 - 5.97 |
| Sherkatolabbasieh et al (23) |
Khorramabad |
2022 |
63 |
30 |
47.62 |
34.88 - 60.59 |
Note. CI: Confidence interval.
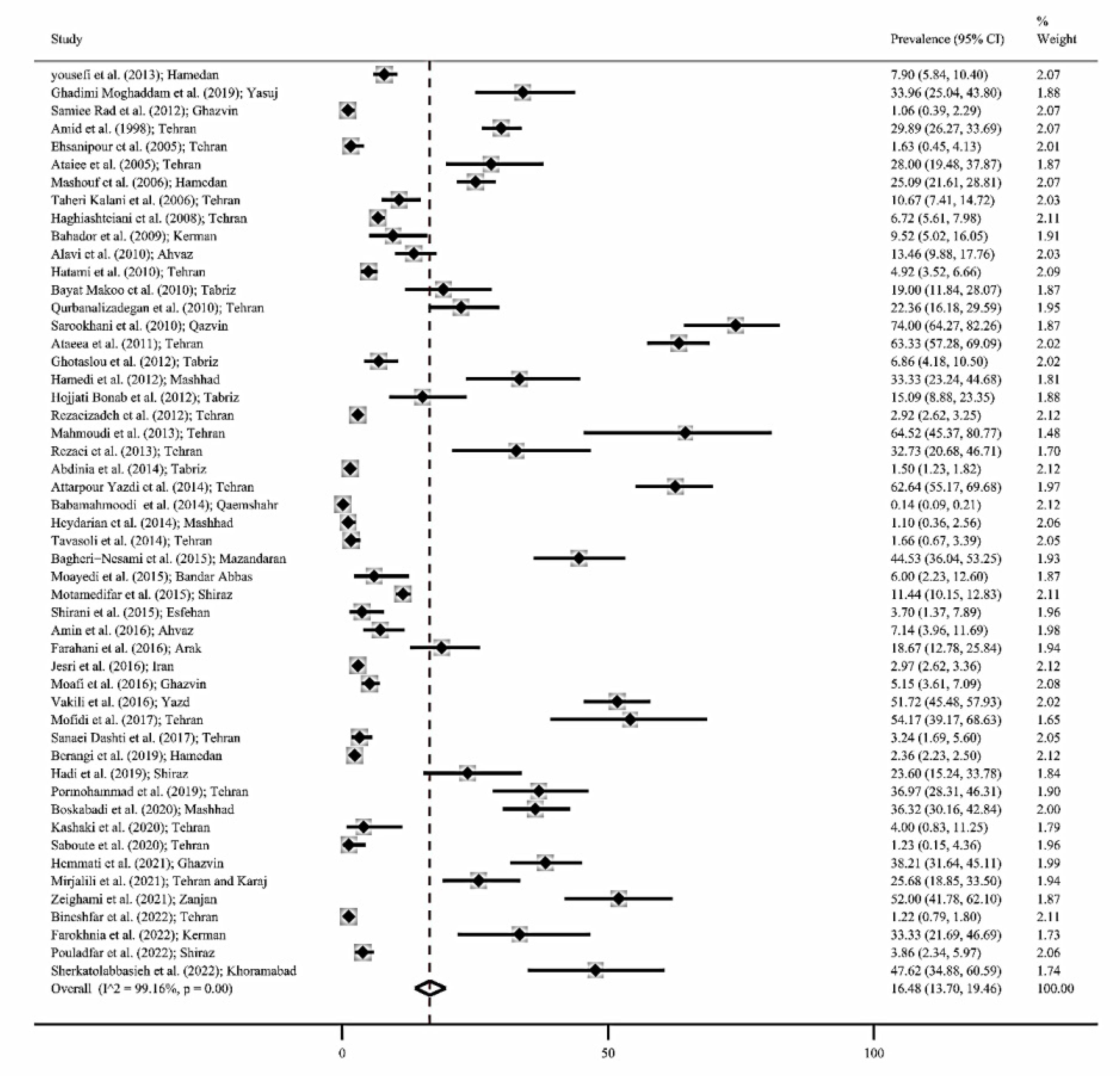
Figure 3.
Forest Plot of Prevalence of Meningitis in Iran
.
Forest Plot of Prevalence of Meningitis in Iran
Etiology of Bacterial Meningitis
In this section, we included 48 articles, 41 of which overlapped with the epidemiology section, and 7 articles (68-74) specifically examined etiology. A total of 1787 gram-positive and 1376 gram-negative bacteria were identified morphologically. Bacteria reported only as a genus (e.g., Enterococcus, Klebsiella, or Acinetobacter) without a species name were excluded from the analysis. S. pneumoniae, H. influenza (mostly type b), N. meningitides, and Escherichia coli were reported in more than 60% of the articles. Table 2 lists bacterial species identified in at least five articles. S. pneumoniae was the cause of 27.89% of cases across 32 studies and was identified as the main cause of bacterial meningitis in Iran. Other frequently reported bacteria included H. influenza, Staphylococcus epidermidis, Klebsiella pneumoniae, N. meningitidis, and Streptococcus agalactiae.
Table 2.
The Most Common Types of Bacterial Meningitis in Iran
|
Organism
|
Study Number
|
Prevalence
(CI 95%)
|
P
Value
|
I2
%
|
|
S. pneumoniae
|
38 |
27.89
(23.26 - 32.74) |
< 0.001 |
85.23 |
|
H. influenzae
|
36 |
15.96
(12.21 - 20.06) |
< 0.001 |
83.59 |
|
S. epidermidis
|
7 |
15.88
(5.35 - 30.27) |
< 0.001 |
94.97 |
|
K. pneumoniae
|
8 |
15.56
(6.61 - 27.01) |
< 0.001 |
88.39 |
|
N. meningitidis
|
29 |
13.13
(9.27 - 17.48) |
< 0.001 |
88.27 |
|
S. agalactiae
|
6 |
11.42
(6.15 - 17.96) |
< 0.001 |
77.33 |
|
E. coli
|
25 |
7.07
(4.84 - 9.61) |
< 0.001 |
66.49 |
|
S. aureus
|
16 |
6.15
(4.09 - 8.52) |
< 0.001 |
57.34 |
|
P. aeruginosa
|
15 |
4
(2.49 - 5.76) |
< 0.001 |
47.21 |
Note. CI: Confidence interval; S. pneumoniae: Streptococcus pneumoniae; H. influenzae: Haemophilus influenzae; S. epidermidis: Staphylococcus epidermidis; K. pneumoniae: Klebsiella pneumoniae; Neisseria meningitidis: N. meningitidis; S. agalactiae: Streptococcus agalactiae; E. coli: Escherichia coli; S. aureus; Staphylococcus aureus; P. aeruginosa; Pseudomonas aeruginosa.
Clinical Manifestations
As shown in Table 3, fever was the most common symptom, observed in 89.37% of patients with meningitis. Nausea, neck stiffness, vomiting, and headache were observed in approximately half of the patients. A quarter (25.42%) of patients had seizures. Other common symptoms, such as jaundice, cerebral edema, cough, and photosensitivity, were reported in fewer than five studies.
Table 3.
Prevalence of Clinical Manifestations in Patients with Bacterial Meningitis
|
Clinical Manifestation
|
Study Number
|
Diagnosis With Meningitis
|
Patient With Manifestation
|
Prevalence
(95% CI)
|
Weight (%)
|
I2
|
P
value
|
| Headache |
8 |
538 |
199 |
44.04 |
11.21 |
94.10 |
< 0.001 |
| Nausea |
6 |
419 |
216 |
55.81 |
10.96 |
92.55 |
< 0.001 |
| Vomiting |
5 |
362 |
164 |
46.58 |
6.84 |
94.53 |
< 0.001 |
| Neck stiffness |
6 |
288 |
125 |
50.60 |
5.75 |
93.99 |
< 0.001 |
| Fever |
9 |
566 |
511 |
89.37 |
46.67 |
90.12 |
< 0.001 |
| Seizure |
9 |
493 |
108 |
25.42 |
18.57 |
91.36 |
< 0.001 |
Note. CI: Confidence interval.
Discussion
This review collected information on the epidemiology and etiology of bacterial meningitis in Iran across all age groups. The articles were about all types of meningitis; however, most studies did not specify the subtype of meningitis, which may be due to the lack of clarity about the exact onset of symptoms. Furthermore, bacteria associated with acute meningitis may be seen in non-acute types, making diagnosis difficult (20). However, for several reasons, it can be argued that our results were related to the acute type of meningitis: (a) Bacteria usually cause acute meningitis; in contrast, subacute and chronic types are mostly associated with fungi, other systemic diseases, and some unusual bacteria (1,75,76). On the other hand, one-third of chronic cases remain undiagnosed, so the number of chronic diagnoses is generally lower (77). (b) Chronic infectious meningitis cases generally occur in immunocompromised individuals, such as HIV patients or those taking immunosuppressive drugs (78). These cases were not included in our article. (c) Mycobacterium tuberculosis, Leptospira, Brucella, and Treponema pallidum are the most commonly known causes of subacute meningitis (75,78). In our search, only two studies reported Brucella, and three reported Mycobacterium tuberculosis. This may be attributed to limited attention given to these bacteria due to the small number of cases and challenges associated with their laboratory culture.
The hospital-associated epidemiology of bacterial meningitis in Iran was 16.48%, which varied significantly between regions and even within cities. In Tehran, reported prevalence ranged from 1.63% to 63.33% (27,37). On the other hand, all four studies conducted in Tabriz reported a prevalence of less than 20% (35,38,40,44). The two studies from Ahvaz showed lower prevalence rates of 13.46% and 7.14% (33,52). These differences in reporting may be due to variations in population characteristics, sample size, diagnostic accuracy, and hygiene levels across cities. To accurately determine the epidemiology of meningitis in an area, studies with a wide range and large sample sizes must be conducted to obtain reliable data. In a three-year study in Taiwan, among 1803 children under five years of age, 13.5% had bacterial meningitis, which is close to the figure reported in our paper (79).
S. pneumoniae was the predominant species causing bacterial meningitis in Iran. This result is consistent with similar studies published in 2015 (80) and 2017 (14) in Iran. In general, this bacterium has long been recognized as a major cause of bacterial meningitis (15,81,82). Similarly, H. influenzae was the second most common species in Iran, with a frequency of 15.96%. Although this bacterium is still a common strain of meningitis (82), its prevalence continues to decline. In the past, H. influenzae was the most frequently reported bacterium in meningitis cases; however, with the introduction of vaccination, its incidence has decreased (83). It should be noted that the pneumococcal vaccine for S. pneumoniae is available in Iran, but its administration is not mandatory within the country’s health program (84). Based on the report in this article and the notably high prevalence of this bacterium among meningitis patients, vaccination is recommended for all children in Iran. Although S. epidermidis and Klebsiella pneumoniae were reported in a limited number of studies, they accounted for more than 15% of the cases in those studies. Coagulase-negative staphylococci have also been identified as serious bacteria in cases of bacterial meningitis in Iran (14,80), but the specific species were not always mentioned. This article highlights S. epidermidis as the most important species. Given that S. epidermidis is a major cause of hospital-acquired infections, it can be inferred that most patients may have been infected in the hospital (85). Other species of this group, such as S. haemolyticus and S. saprophyticus, were also reported in the reviewed articles.
The prevalence of K. pneumoniae was found to be higher than previously reported. This increase might be due to the inclusion of a larger number of adult patients in this review, as this bacterium is recognized as a major cause of meningitis in adults (86). Furthermore, the reduction in incidence of primary causative agents of bacterial meningitis due to widespread vaccination may have led to an increase in the reported prevalence of other bacteria.
Neisseria meningitidis is a leading cause of bacterial meningitis in many parts of the world, especially in America, Europe, and Africa (6,15). However, it is less prevalent in Iran. This article reported a rate of 13.13%, which is consistent with other previous studies in Iran, showing prevalence rates of 13% (14) and 10.5% (80). This could be due to three reasons: (a) N. meningitidis is commonly seen in meningitis among young adults, while Iranian studies often do not focus on this age group (87). (b) Most cases of N. meningitidis are reported in the meningitis belt of Africa. Given the differences in climate, ethnicity, and healthcare infrastructure between Iran and these countries, differences in the predominant types of meningitis are not surprising (88). (c) The development of the meningococcal vaccine has naturally led to a reduction in the rate of its infection.(59) S. agalactiae and E. coli were also significantly reported in Iran. Given that there is no vaccine in the national health program for meningitis caused by these two bacteria (13,89), it can be predicted that their prevalence may increase in the future. It should be noted that S. agalactiae is now considered one of the leading causes of meningitis, especially in children (90,91).
In a 2015 review conducted in Iran, Enterobacter was reported as the third most common cause of meningitis, accounting for 12.24% of cases (80). In our study, a significant number of articles mentioned Enterobacter but not a specific species. Listeria monocytogenes was uncommon in this review, likely because this bacterium more commonly causes meningitis in infants, patients over 50 years of age, and those with weakened immune systems (91). The clinical manifestations are usually similar across different types of meningitis. In this review, fever was observed in about 90% of patients. About 50% of cases presented with nausea, neck stiffness, vomiting, and headache, in respective order of frequency. The classical triad of meningitis (i.e., fever, stiff neck, and altered mental status) is most commonly observed in people over 60 years of age and occurs in only 40% of cases overall (92). The triad, along with headache, constitutes the classical manifestations of meningitis, and nearly every patient presenting with at least two of these symptoms (93). The high incidence of nausea and vomiting in this review may be due to the younger age of most patients, as these symptoms are more common in children (6,14). This pattern is to some extent similar to a study conducted on Iranian children with bacterial meningitis, in which fever was reported in 71% of cases and nausea and vomiting in 67%, which supports our findings (14). Another study on bacterial meningitis across all age groups reported fever in 95% of cases, vomiting in 57%, and seizures in only 12%. Across all studies, fever remains the most consistent clinical symptom (94).
A study of bacterial meningitis in adults (6) reported headache and neck stiffness frequently (in more than 80% of cases) and seizures in only 5%. In this review, 25% of patients had seizures, indicating a higher seizure prevalence in children than in adults with meningitis. Altered mental status was not widely reported in our study. Sleepiness, restlessness, and irritability were observed in some patients as nonspecific neurological symptoms, which are also seen in younger meningitis patients.
Limitations
This study has several limitations. First, a significant number of bacterial reports (over 500) lacked species-level identification, being reported only at the genus level or left unspecified. These cases were excluded from the analysis, which may have introduced bias and reduced the statistical power of the findings. Second, most of the included studies were conducted in Tehran, while data from many other cities were either limited or unavailable. Given the differences in climate, cultural practices, and hygiene standards across various regions of Iran, the lack of comprehensive geographic representation may have influenced the generalizability of the results. Lastly, inclusion in this review required a positive CSF culture result. Although CSF culture is considered the gold standard for diagnosing bacterial meningitis, it has a reported false-negative rate of 10–30% (81,94). Therefore, some cases of bacterial meningitis may have been missed, potentially underestimating the true burden of the disease.
Conclusion
This article provides valuable insights into the burden and etiology of hospital-based bacterial meningitis in Iran. The results highlight the need for vaccination and improved diagnostic efforts to identify regional differences and address healthcare inequalities. To better understand the national burden of disease, future studies should not be limited to hospitalized cases but should also include population-based data from across the country. Moreover, implementing and evaluating nationwide vaccination strategies, especially against pneumococcal disease, alongside strengthening surveillance systems and broadening study coverage, could substantially improve prevention efforts and inform more effective public health planning.
Competing Interests
The authors declare that they have no conflict of interests.
Ethical Approval
Not applicable.
Funding
This study was funded by Ilam University of Medical Sciences, Ilam, Iran, under grant number IR.MEDILAM.REC.1402.298.
References
- Coyle PK. Overview of acute and chronic meningitis. Neurol Clin 1999; 17(4):691-710. doi: 10.1016/s0733-8619(05)70162-6 [Crossref] [ Google Scholar]
- Ginsberg L, Kidd D. Chronic and recurrent meningitis. Pract Neurol 2008; 8(6):348-61. doi: 10.1136/jnnp.2008.157396 [Crossref] [ Google Scholar]
- Helbok R, Broessner G, Pfausler B, Schmutzhard E. Chronic meningitis. J Neurol 2009; 256(2):168-75. doi: 10.1007/s00415-009-0122-0 [Crossref] [ Google Scholar]
- Kumar R. Aseptic meningitis: diagnosis and management. Indian J Pediatr 2005; 72(1):57-63. doi: 10.1007/bf02760582 [Crossref] [ Google Scholar]
- Shukla B, Aguilera EA, Salazar L, Wootton SH, Kaewpoowat Q, Hasbun R. Aseptic meningitis in adults and children: diagnostic and management challenges. J Clin Virol 2017; 94:110-4. doi: 10.1016/j.jcv.2017.07.016 [Crossref] [ Google Scholar]
- van de Beek D, de Gans J, Spanjaard L, Weisfelt M, Reitsma JB, Vermeulen M. Clinical features and prognostic factors in adults with bacterial meningitis. N Engl J Med 2004; 351(18):1849-59. doi: 10.1056/NEJMoa040845 [Crossref] [ Google Scholar]
- Doherty CM, Forbes RB. Diagnostic lumbar puncture. Ulster Med J 2014; 83(2):93-102. [ Google Scholar]
- Shokrollahi MR, Shabanzadeh K, Noorbakhsh S, Tabatabaei A, Movahedi Z, Shamshiri AR. Diagnostic value of CRP, procalcitonin, and ferritin levels in cerebrospinal fluid of children with meningitis. Cent Nerv Syst Agents Med Chem 2018; 18(1):58-62. doi: 10.2174/1871524916666160302103223 [Crossref] [ Google Scholar]
- Tunkel AR, Hartman BJ, Kaplan SL, Kaufman BA, Roos KL, Scheld WM. Practice guidelines for the management of bacterial meningitis. Clin Infect Dis 2004; 39(9):1267-84. doi: 10.1086/425368 [Crossref] [ Google Scholar]
- Al-Qahtani SM, Shati AA, Alqahtani YA, Ali AS. Etiology, clinical phenotypes, epidemiological correlates, laboratory biomarkers and diagnostic challenges of pediatric viral meningitis: descriptive review. Front Pediatr 2022; 10:923125. doi: 10.3389/fped.2022.923125 [Crossref] [ Google Scholar]
- Hoffman O, Weber RJ. Pathophysiology and treatment of bacterial meningitis. Ther Adv Neurol Disord 2009; 2(6):1-7. doi: 10.1177/1756285609337975 [Crossref] [ Google Scholar]
- Jarrin I, Sellier P, Lopes A, Morgand M, Makovec T, Delcey V. Etiologies and management of aseptic meningitis in patients admitted to an internal medicine department. Medicine (Baltimore) 2016; 95(2):e2372. doi: 10.1097/md.0000000000002372 [Crossref] [ Google Scholar]
- World Health Organization (WHO). Meningococcal Meningitis: Fact Sheet 2017. WHO; 2017.
- Houri H, Pormohammad A, Riahi SM, Nasiri MJ, Fallah F, Dabiri H. Acute bacterial meningitis in Iran: systematic review and meta-analysis. PLoS One 2017; 12(2):e0169617. doi: 10.1371/journal.pone.0169617 [Crossref] [ Google Scholar]
- Oordt-Speets AM, Bolijn R, van Hoorn RC, Bhavsar A, Kyaw MH. Global etiology of bacterial meningitis: a systematic review and meta-analysis. PLoS One 2018; 13(6):e0198772. doi: 10.1371/journal.pone.0198772 [Crossref] [ Google Scholar]
- Herzog R, Álvarez-Pasquin MJ, Díaz C, Del Barrio JL, Estrada JM, Gil Á. Are healthcare workers’ intentions to vaccinate related to their knowledge, beliefs and attitudes? A systematic review. BMC Public Health 2013; 13:154. doi: 10.1186/1471-2458-13-154 [Crossref] [ Google Scholar]
- Sarookhani MR, Ayazi P, Alizadeh S, Foroughi F, Sahmani A, Adineh M. Comparison of 16S rDNA-PCR amplification and culture of cerebrospinal fluid for diagnosis of bacterial meningitis. Iran J Pediatr 2010; 20(4):471-5. [ Google Scholar]
- Heydarian F, Ashrafzadeh F, Rostazadeh A. Predicting factors and prevalence of meningitis in patients with first seizure and fever aged 6 to 18 months. Neurosciences (Riyadh) 2014; 19(4):297-300. [ Google Scholar]
- Amid MH. A spinal fluid scoring system for differentiation of bacterial and viral meningitis. J Res Med Sci 1998;22(3):47-54. [Persian].
- Bineshfar N, Rezaei A, Mirahmadi A, Shokouhi S, Gharehbagh FJ, Haghighi M. Evaluation of the epidemiologic, clinical, radiologic, and treatment methods of patients with subacute and chronic meningitis. BMC Neurol 2022; 22(1):340. doi: 10.1186/s12883-022-02873-1 [Crossref] [ Google Scholar]
- Farokhnia M, Hosseininasab A, Kamali M, Pourabbas B, Taheri Sarvtin M. A study on bacterial agents of patients with meningitis referred to Afzalipour hospital in Kerman, south-east Iran. Int J Med Lab 2022; 9(1):1-5. doi: 10.18502/ijml.v9i1.9080 [Crossref] [ Google Scholar]
- Pouladfar G, Sanaei Dashti A, Kadivar MR, Jafari M, Pourabbas B, Jamalidoust M. Evaluation of multiplex real-time PCR and WHO criteria for diagnosing childhood bacterial meningitis in a tertiary referral hospital in Iran. Arch Pediatr Infect Dis 2022; 10(3):e101822. doi: 10.5812/pedinfect.101822 [Crossref] [ Google Scholar]
- Sherkatolabbasieh HR, Shakib P, Khademi N, Rezaei F. Epidemiological evaluation of meningitis in hospitalized patients in shahid Madani hospital in Khorramabad. Yafteh 2022;23(5):41-51. [Persian].
- Yousefi Mashouf R, Hashemi H, Shams S. Study of bacterial agents of meningitis in children and detection of antibiogram patterns in Hamadan. Yafteh 2004;5(2):31-9. [Persian].
- Ghadimi Moghaddam A, Ghatee MA, Keshtkari A, Shabankareh M. Prevalence of bacterial causes of meningitis and related factors in patients admitted to Imam Sajjad hospital in Yasuj. Armaghane Danesh 2019;24(5):853-64. [Persian].
- Samiee-Rad F, Karimfar MH. Prevalence of newborn bacterial meningitis in Kosar hospital 2007-2012. J Zabol Univ Med Sci 2012;4(1):49-57. [Persian].
- Ehsanipour F, Khodapanahandeh F, Aslani Z. The prevalence of meningitis in children with febrile seizure hospitalized at Hazrat Rasoul hospital (1997-2002). Razi J Med Sci 2005;11(44):907-11. [Persian].
- Ataei RA, Mehrabi TA, Ghorbani GH, Karimi Zarchi AA, Hajia M, Hosseini SM, et al. Determination of bacterial etiology of 100 CSF samples of patients with meningitis at four military hospitals in Tehran between 2003 and 2005. J Mil Med 2005;7(1):49-56. [Persian].
- Yousefi Mashouf R, Hashemi SH, Bijarchi M. Bacterial agents of meningitis in children and detection of their antibiotic resistance patterns in Hamadan, Western Iran. Pak J Biol Sci 2006; 9(7):1293-8. [ Google Scholar]
- Taheri Kalani M, Akbari Nakhjavani N, Kazemi B, Bonakdar Hashemi F, Haghi-Ashtiani MT, Nouri K, et al. Survey rate isolation of Heamophilus influenzae type B in CSF of pediatrics suspected to meningitis by culture and PCR in Tehran Center of Medical Children. Tehran Univ Med J 2006;63(12):1006-14. [Persian].
- Haghi-Ashtiani MT, Mohammadi-Yeganeh S, Soroush S, Sadeghifard N, Sayadi S, Dabyri H. Frequency and antimicrobial susceptibility of Haemophilus influenzae type B isolated from children suspected to meningitis. Iran J Public Health 2008; 37(4):52-8. [ Google Scholar]
- Bahador M, Amini M, Bahador M. Common cause and cerebrospinal fluid changes of acute bacterial meningitis. Iran J Pathol 2009; 4(2):75-9. [ Google Scholar]
- Alavi SM, Moshiri N, Shokri S. Evaluation of epidemiological, clinical and laboratory findings of admitted patients with meningitis in infectious diseases ward of Razi hospital, Ahvaz. Sci Med J 2010;9(3):221-31. [Persian].
- Hatami H, Hatami M, Soori H, Janbakhsh AR, Mansouri F. Epidemiological, clinical, and laboratory features of brucellar meningitis. Arch Iran Med 2010; 13(6):486-91. [ Google Scholar]
- Bayat Makoo Z, Soltani HR, Hasani A, Bayat Makoo R, Mashrabi O. Diagnostic value of serum and cerebrospinal fluid procalcitonin in differentiation bacterial from aseptic meningitis. Am J Infect Dis 2010; 6(4):93-7. doi: 10.3844/ajidsp.2010.93.97 [Crossref] [ Google Scholar]
- Qurbanalizadegan M, Ranjbar R, Ataee R, Hajia M, Goodarzi Z, Farshad S. Specific PCR assay for rapid and direct detection of Neisseria meningitidis in cerebrospinal fluid specimens. Iran J Public Health 2010; 39(4):45-50. [ Google Scholar]
- Ataee RA, Mehrabi-Tavana A, Izadi M, Hosseini SM, Ataee MH. Bacterial meningitis: a new risk factor. J Res Med Sci 2011; 16(2):207-10. [ Google Scholar]
- Ghotaslou R, Farajnia S, Yeganeh F, Abdoli-Oskouei S, Ahangarzadeh Rezaee M, Barzegar M. Detection of acute childhood meningitis by PCR, culture and agglutination tests in Tabriz, Iran. Acta Med Iran 2012; 50(3):192-6. [ Google Scholar]
- Hamedi A, Ayatollahi H, Ataee Nakhaee A. Evaluation of IL-6 and high sensitive C reactive protein value in CSF and serum children suspected meningitis referred to pediatric emergency room. Iran Red Crescent Med J 2012; 14(12):822-5. doi: 10.5812/ircmj.4726 [Crossref] [ Google Scholar]
- Hojjati Bonab Z, Farajnia S, Ghotaslou R, Nikkhah E. Evaluation of nested PCR method for diagnosis of meningitis due to Neisseria meningitidis and Haemophilus influenzae. Turk J Biol 2012; 36(6):727-31. doi: 10.3906/biy-1111-27 [Crossref] [ Google Scholar]
- Rezaeizadeh G, Pourakbari B, Ashtiani MH, Asgari F, Mahmoudi S, Mamishi S. Antimicrobial susceptibility of bacteria isolated from cerebrospinal fluids in an Iranian referral pediatric center, 1998-2008. Maedica (Bucur) 2012; 7(2):131-7. [ Google Scholar]
- Mahmoudi S, Zandi H, Pourakbari B, Ashtiani MT, Mamishi S. Acute bacterial meningitis among children admitted into an Iranian referral children’s hospital. Jpn J Infect Dis 2013; 66(6):503-6. doi: 10.7883/yoken.66.503 [Crossref] [ Google Scholar]
- Rezaei M, Mamishi S, Mahmoudi S, Pourakbari B, Khotaei G, Daneshjou K. Cerebrospinal fluid ferritin in children with viral and bacterial meningitis. Br J Biomed Sci 2013; 70(3):101-3. doi: 10.1080/09674845.2013.11669943 [Crossref] [ Google Scholar]
- Abdinia B, Ahangarzadeh Rezaee M, Abdoli Oskouie S. Etiology and antimicrobial resistance patterns of acute bacterial meningitis in children: a 10-year referral hospital-based study in northwest Iran. Iran Red Crescent Med J 2014; 16(7):e17616. doi: 10.5812/ircmj.17616 [Crossref] [ Google Scholar]
- Attarpour-Yazdi MM, Ghamarian A, Mousaviehzadeh M, Davoudi N. Identification of the serotypes of bacterial meningitis agents; implication for vaccine usage. Iran J Microbiol 2014; 6(4):211-8. [ Google Scholar]
- Babamahmoodi F, Davoudi A, Babamahmoodi A, Sepehri Manesh M. Epidemiologic characteristics of patients treated in a referral center with the diagnosis of central nervous system infection in north of Iran, from March 2008 to March 2012: a retrospective observational registry study. Arch Neurosci 2014; 1(2):82-7. doi: 10.5812/archneurosci.13894 [Crossref] [ Google Scholar]
- Tavasoli A, Afsharkhas L, Edraki A. Frequency of meningitis in children presenting with febrile seizures at Ali-Asghar Children’s Hospital. Iran J Child Neurol 2014; 8(4):51-6. [ Google Scholar]
- Bagheri-Nesami M, Babamahmoodi F, Nikkhah A. Types, risk factors, clinical symptoms and diagnostic tests of acute adult meningitis in northern Iran during 2006-2012. J Clin Diagn Res 2015; 9(5):IC01-5. doi: 10.7860/jcdr/2015/11991.5936 [Crossref] [ Google Scholar]
- Moayedi AR, Nejatizadeh A, Mohammadian M, Rahmati MB, Namardizadeh V. Accuracy of universal polymerase chain reaction (PCR) for detection of bacterial meningitis among suspected patients. Electron Physician 2015; 7(8):1609-12. doi: 10.19082/1609 [Crossref] [ Google Scholar]
- Motamedifar M, Sedigh Ebrahim-Saraie H, Mansury D, Nikokar I, Hashemizadeh Z. Prevalence of etiological agents and antimicrobial resistance patterns of bacterial meningitis in Nemazee hospital, Shiraz, Iran. Arch Clin Infect Dis 2015; 10(2):e22703. doi: 10.5812/archcid.22703 [Crossref] [ Google Scholar]
- Shirani K, Talaei Z, Yaran M, Ataei B, Mehrabi-Koushki A, Khorvash F. Diagnosed tuberculous meningitis using cerebrospinal fluid polymerase chain reaction in patients hospitalized with the diagnosis of meningitis in referral hospitals in Isfahan. J Res Med Sci 2015; 20(3):224-7. [ Google Scholar]
- Amin M, Ghaderpanah M, Navidifar T. Detection of Haemophilus influenzae type B, Streptococcus agalactiae, Streptococcus pneumoniae and Neisseria meningitidis in CSF specimens of children suspicious of meningitis in Ahvaz, Iran. Kaohsiung J Med Sci 2016; 32(10):501-6. doi: 10.1016/j.kjms.2016.08.009 [Crossref] [ Google Scholar]
- Farahani H, Ghaznavi-Rad E, Mondanizadeh M, MirabSamiee S, Khansarinejad B. Specific detection of common pathogens of acute bacterial meningitis using an internally controlled tetraplex-PCR assay. Mol Cell Probes 2016; 30(4):261-5. doi: 10.1016/j.mcp.2016.07.002 [Crossref] [ Google Scholar]
- Jesri N, Rezaei F, Saghafipour A, Asghari H, Noroozei M. Spatial analysis of bacterial meningitis in Iran using geographical information system. J Mazandaran Univ Med Sci 2016;25(132):309-14. [Persian].
- Moafi N, Issazadeh K. Frequency of neonatal and children bacterial meningitis and determining their antibiotic sensitivity patterns in hospitals of Iran. Int J Mol Clin Microbiol 2016; 6(1):608-12. [ Google Scholar]
- Vakili M, Rostami Z, Mirzaei M. Evaluation of the laboratory, epidemiological and clinical characteristics of meningitis patients admitted to the hospitals of Yazd from 2009 to 2013. Int J Med Lab 2016;3(4):221-8. [Persian].
- Mofidi M, Negaresh N, Farsi D, Rezai M, Mahshidfar B, Abbasi S. Jolt accentuation and its value as a sign in diagnosis of meningitis in patients with fever and headache. Turk J Emerg Med 2017; 17(1):29-31. doi: 10.1016/j.tjem.2016.11.001 [Crossref] [ Google Scholar]
- Sanaei Dashti A, Alizadeh S, Karimi A, Khalifeh M, Shoja SA. Diagnostic value of lactate, procalcitonin, ferritin, serum-C-reactive protein, and other biomarkers in bacterial and viral meningitis: a cross-sectional study. Medicine (Baltimore) 2017; 96(35):e7637. doi: 10.1097/md.0000000000007637 [Crossref] [ Google Scholar]
- Berangi Z, Karami M, Mohammadi Y, Nazarzadeh M, Zahraei SM, Javidrad H. Epidemiological profile of meningitis in Iran before pentavalent vaccine introduction. BMC Pediatr 2019; 19(1):370. doi: 10.1186/s12887-019-1741-y [Crossref] [ Google Scholar]
- Hadi N, Bagheri K. A five-year retrospective multicenter study on etiology and antibiotic resistance pattern of bacterial meningitis among Iranian children. Infect Epidemiol Microbiol 2019; 5(4):17-24. [ Google Scholar]
- Pormohammad A, Lashkarbolouki S, Azimi T, Gholizadeh P, Bostanghadiri N, Safari H. Clinical characteristics and molecular epidemiology of children with meningitis in Tehran, Iran: a prospective study. New Microbes New Infect 2019; 32:100594. doi: 10.1016/j.nmni.2019.100594 [Crossref] [ Google Scholar]
- Boskabadi H, Heidari E, Zakerihamidi M. Etiology, clinical findings and laboratory parameters in neonates with acute bacterial meningitis. Iran J Microbiol 2020; 12(2):89-97. [ Google Scholar]
- Kashaki M, Norouzi E, Heidarali S, Mohagheghi P, Soltani M, Karbalaei Hasani H. Is there any correlation between cerebrospinal fluid and serum C-reactive protein in neonates suspected to meningitis?. J Kerman Univ Med Sci 2020; 27(5):389-93. doi: 10.22062/jkmu.2020.91471.[Persian] [Crossref] [ Google Scholar]
- Saboute M, Kashaki M, Yavar R, Bordbar A, Khalessi N, Allahqoli L. Prevalence of meningitis among hospitalized neonates with urinary tract infection. Iran J Neonatol 2020; 11(2):66-71. doi: 10.22038/ijn.2020.41257.1677 [Crossref] [ Google Scholar]
- Hemmati N, Nikkhahi F, Javadi A, Eskandarion S, Marashi SM. Use of a new multiplex quantitative polymerase chain reaction-based assay for simultaneous detection of Neisseria meningitidis, Escherichia coli K1, Streptococcus agalactiae, and Streptococcus pneumoniae. Iran J Microbiol 2021; 13(4):464-9. doi: 10.18502/ijm.v13i4.6970 [Crossref] [ Google Scholar]
- Mirjalili A, Mollazadeh SH. Molecular epidemiology study of suspected meningitis cases in Tehran and Alborz provinces. J Adv Biomed Sci 2021; 11(3):3976-83. doi: 10.18502/jabs.v11i3.8791 [Crossref] [ Google Scholar]
- Zeighami H, Roudashti S, Bahari S, Haghi F, Hesami N. Frequency of etiological agents of acute bacterial meningitis using culture and polymerase chain reaction assay. New Microbes New Infect 2021; 43:100930. doi: 10.1016/j.nmni.2021.100930 [Crossref] [ Google Scholar]
- Tabatabaie P, Sayahtaheri S, Siadati A, Alizad O. Etiology and neurological complications of bacterial meningitis in 189 patients. Acta Med Iran 1997; 35(1-2):33-8. [ Google Scholar]
- Aletayeb MH, Farajzadeh Sheikh A, Dehdashtian M. Eleven-year study of causes of neonatal bacterial meningitis in Ahvaz, Iran. Pediatr Int 2010; 52(3):463-6. doi: 10.1111/j.1442-200X.2010.03107.x [Crossref] [ Google Scholar]
- Haghi-Ashtiani MT, Mamishi S, Shayanfar N, Mohammadpour M, Yaghmaei B, Abedini M. Antimicrobial susceptibility profiles associated with bacterial meningitis among children: a referral hospital-based study in Iran. Acta Microbiol Immunol Hung 2011; 58(4):273-8. doi: 10.1556/AMicr.58.2011.4.3 [Crossref] [ Google Scholar]
- Khalessi N, Afsharkhas L. Neonatal meningitis: risk factors, causes, and neurologic complications. Iran J Child Neurol 2014; 8(4):46-50. [ Google Scholar]
- Heydari B, Khalili H, Karimzadeh I, Emadi-Kochak H. Clinical, paraclinical, and antimicrobial resistance features of community-acquired acute bacterial meningitis at a large infectious diseases ward in Tehran, Iran. Iran J Pharm Res 2016; 15(1):347-54. [ Google Scholar]
- Mohsenipour R, Gharib B, Eshaghi H, Rahmani P. Antibiotic susceptibility of bacterial agents causing meningitis in children older than 1 month. Drug Res (Stuttg) 2020; 70(4):174-7. doi: 10.1055/a-1112-7006 [Crossref] [ Google Scholar]
- Keshavarz Valian S, Mahmoudi S, Pourakbari B, Banar M, Haghi-Ashtiani MT, Mamishi S. The causative organisms of bacterial meningitis and their antimicrobial resistance profiles in Iranian children in 2011-2016. Infect Disord Drug Targets 2020; 20(2):229-36. doi: 10.2174/1871526519666181123130101 [Crossref] [ Google Scholar]
- Zunt JR, Baldwin KJ. Chronic and subacute meningitis. Continuum (Minneap Minn) 2012; 18(6):1290-318. doi: 10.1212/01.Con.0000423848.17276.21 [Crossref] [ Google Scholar]
- Sulaiman T, Salazar L, Hasbun R. Acute versus subacute community-acquired meningitis: analysis of 611 patients. Medicine (Baltimore) 2017; 96(36):e7984. doi: 10.1097/md.0000000000007984 [Crossref] [ Google Scholar]
- Hildebrand J, Aoun M. Chronic meningitis: still a diagnostic challenge. J Neurol 2003; 250(6):653-60. doi: 10.1007/s00415-003-1101-5 [Crossref] [ Google Scholar]
- Thakur KT, Wilson MR. Chronic Meningitis. Continuum (Minneap Minn) 2018; 24(5):1298-326. doi: 10.1212/con.0000000000000664 [Crossref] [ Google Scholar]
- Nguyen DT, Nguyen TL, Olmsted A, Duong TH, Hoang HM, Nguyen LH. Epidemiology of pneumococcal meningitis in sentinel hospital surveillance of Viet Nam, 2015-2018. BMC Infect Dis 2024; 24(1):1179. doi: 10.1186/s12879-024-10065-0 [Crossref] [ Google Scholar]
- Ghotaslou R, Yeganeh-Sefidan F, Salahi-Eshlaqi B, Ebrahimzadeh-Leylabadlo H. Etiology of acute bacterial meningitis in Iran: a systematic review. Acta Med Iran 2015; 53(8):454-61. [ Google Scholar]
- Durand ML, Calderwood SB, Weber DJ, Miller SI, Southwick FS, Caviness VS Jr. Acute bacterial meningitis in adults A review of 493 episodes. N Engl J Med 1993; 328(1):21-8. doi: 10.1056/nejm199301073280104 [Crossref] [ Google Scholar]
- Ali M, Chang BA, Johnson KW, Morris SK. Incidence and aetiology of bacterial meningitis among children aged 1-59 months in South Asia: systematic review and meta-analysis. Vaccine 2018; 36(39):5846-57. doi: 10.1016/j.vaccine.2018.07.037 [Crossref] [ Google Scholar]
- Martin M, Casellas JM, Madhi SA, Urquhart TJ, Delport SD, Ferrero F. Impact of haemophilus influenzae type b conjugate vaccine in South Africa and Argentina. Pediatr Infect Dis J 2004; 23(9):842-7. doi: 10.1097/01.inf.0000137575.82874.0c [Crossref] [ Google Scholar]
- Rafiei Tabatabaei S, Shamshiri AR, Nasiri MJ, Weinberger DM, Dadashi M, Karimi A. Pneumococcal meningitis in Iran: a systematic review and meta–analysis. J Acute Dis 2019; 8(3):99-105. doi: 10.4103/2221-6189.259108 [Crossref] [ Google Scholar]
- Noguchi T, Nagao M, Yamamoto M, Matsumura Y, Kitano T, Takaori-Kondo A. Staphylococcus epidermidis meningitis in the absence of a neurosurgical device secondary to catheter-related bloodstream infection: a case report and review of the literature. J Med Case Rep 2018; 12(1):106. doi: 10.1186/s13256-018-1646-7 [Crossref] [ Google Scholar]
- Lee PY, Chang WN, Lu CH, Lin MW, Cheng BC, Chien CC. Clinical features and in vitro antimicrobial susceptibilities of community-acquired Klebsiella pneumoniae meningitis in Taiwan. J Antimicrob Chemother 2003; 51(4):957-62. doi: 10.1093/jac/dkg158 [Crossref] [ Google Scholar]
- Bhimraj A. Acute community-acquired bacterial meningitis in adults: an evidence-based review. Cleve Clin J Med 2012; 79(6):393-400. doi: 10.3949/ccjm.79gr.12003 [Crossref] [ Google Scholar]
- Agier L, Martiny N, Thiongane O, Mueller JE, Paireau J, Watkins ER. Towards understanding the epidemiology of Neisseria meningitidis in the African meningitis belt: a multi-disciplinary overview. Int J Infect Dis 2017; 54:103-12. doi: 10.1016/j.ijid.2016.10.032 [Crossref] [ Google Scholar]
- World Health Organization. WHO position paper, meningococcal A conjugate vaccine: updated guidance, February 2015. Vaccine 2018; 36(24):3421-2. doi: 10.1016/j.vaccine.2017.07.063 [Crossref] [ Google Scholar]
- Mehrdadi S. Acute bacterial meningitis: diagnosis, treatment and prevention. J Arch Mil Med 2019; 6(4):e84749. doi: 10.5812/jamm.84749 [Crossref] [ Google Scholar]
- Hasbun R. Progress and challenges in bacterial meningitis: a review. JAMA 2022; 328(21):2147-54. doi: 10.1001/jama.2022.20521 [Crossref] [ Google Scholar]
- van de Beek D, Brouwer MC, Koedel U, Wall EC. Community-acquired bacterial meningitis. Lancet 2021; 398(10306):1171-83. doi: 10.1016/s0140-6736(21)00883-7 [Crossref] [ Google Scholar]
- Tunkel AR, van de Beek D, Scheld WM. Acute meningitis. In: Mandell, Douglas, and Bennett’s Principles and Practice of Infectious Diseases. Elsevier; 2014. p. 1097-138.
- Flores-Cordero JM, Amaya-Villar R, Rincón-Ferrari MD, Leal-Noval SR, Garnacho-Montero J, Llanos-Rodríguez AC. Acute community-acquired bacterial meningitis in adults admitted to the intensive care unit: clinical manifestations, management and prognostic factors. Intensive Care Med 2003; 29(11):1967-73. doi: 10.1007/s00134-003-1935-4 [Crossref] [ Google Scholar]