Avicenna Journal of Clinical Microbiology and Infection. 12(1):10-20.
doi: 10.34172/ajcmi.3620
Original Article
Epidemiological and Clinical Insights into Genotypic Diversity, Antibiotic Resistance Determinants, and Capsular Types of Klebsiella pneumoniae Isolates from Hospitalized Patients in Amol, Northern Iran
Nassim Tavassoli Conceptualization, Data curation, Investigation, Methodology, Writing – original draft, 1 
Fatemeh Zaboli Supervision, Writing – review & editing, 1, *
Rahem Khoshbakht Data curation, Formal analysis, Writing – original draft, 2, *
Mojtaba Khosravi Methodology, Writing – review & editing, 2
Author information:
1Department of Microbiology, Ayatollah Amoli Branch, Islamic Azad University, Amol, Iran
2Department of Pathobiology, Amol University of Special Modern Technologies, Amol, Iran
Abstract
Background: Klebsiella pneumoniae is a Gram-negative opportunistic pathogen and a common cause of nosocomial infections. The present study aimed to investigate the distribution, antibiotic resistance patterns, resistance genes, capsular types, and genotypes of K. pneumoniae isolates.
Methods: A total of 872 clinical samples were collected from inpatients across various hospital wards in Amol, northern Iran. K. pneumoniae isolates were identified and tested for antibiotic susceptibility. Capsular typing and detection of resistance genes were performed, and enterobacterial repetitive intergenic consensus polymerase chain reaction (ERIC-PCR) was used to type the isolates.
Results: K. pneumoniae was isolated from 70 out of 872 samples (8.04%), with the highest prevalence in urine (58.6%) and sputum (25.7%). High resistance rates were observed against erythromycin (98.6%), ampicillin (92.9%), and cefazolin (68.6%), while no resistance to colistin was detected. Multidrug-resistant (MDR) was found in 55.71% of isolates, and 15.71% were extensively drug-resistant (XDR). Carbapenem-resistant K. pneumoniae (CRKP) accounted for 55.7% of the isolates. The most prevalent capsular type was the K57. Forty-eight resistance gene patterns were detected, with the tetB gene present in all isolates, whereas the mcr and blaVEB genes were not detected. ERIC-PCR genotyping revealed 24 different clusters in the phylogenetic dendrogram.
Conclusion: This study highlights the prevalence of antibiotic-resistant K. pneumoniae strains exhibiting significant clonal diversity among isolates from hospital wards in Iran. The findings underscore the need for more stringent infection control measures and management practices related to the misuse of antibiotics to tame the rampant resistant K. pneumoniae in hospitals. These results are compatible with the globally prevailing phenomenon of increased resistance and further emphasize the necessity for sustained, in-depth intelligence-gathering processes and multicenter investigations to decode patterns on a regional and international scale.
Keywords: Klebsiella pneumonia, Antibiotic resistance, Resistance genes, Genotyping
Copyright and License Information
© 2025 The Author(s); Published by Hamadan University of Medical Sciences.
This is an open-access article distributed under the terms of the Creative Commons Attribution License (
https://creativecommons.org/licenses/by/4.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Please cite this article as follows: Tavassoli N, Zaboli F, Khoshbakht R, Khosravi M. Epidemiological and clinical insights into genotypic diversity, antibiotic resistance determinants, and capsular types of Klebsiella pneumoniae isolates from hospitalized patients in Amol, Northern Iran. Avicenna J Clin Microbiol Infect. 2025;12(1):10-20. doi:10.34172/ajcmi.3620
Introduction
Klebsiella pneumoniae is a significant opportunistic pathogen causing a wide range of infections in healthcare settings. This Gram-negative bacterium is associated with high mortality rates among critically ill patients, imposing a substantial financial burden on hospitals (1-4). The presence of multiple resistance genes in gram-negative bacteria affects treatment options and poses broader environmental risks. The rise of antibiotic-resistant K. pneumoniae strains in hospitals has raised concerns globally. These strains are known to cause both community- and hospital-acquired infections and carry a range of antibiotic-resistant genes. Identifying these genes helps understand antibiotic resistance mechanisms and develop targeted therapeutic strategies (5,6).
The global rise in K. pneumoniae resistance has become a critical issue, with hospital-acquired infections caused by multidrug-resistant (MDR) strains leading to increased morbidity and mortality worldwide. In recent years, a significant global shift has been observed globally towards the emergence of carbapenem-resistant K. pneumoniae (CRKP), which poses a serious threat to public health. Studies from various regions, including Europe, Asia, and the Americas, have highlighted the spread of these resistant strains, emphasizing the urgent need for coordinated international efforts in surveillance, prevention, and treatment strategies (1,4,5). These findings underscore the global urgency to address the growing threat of antimicrobial resistance, which aligns with the findings observed in Iranian hospitals.
In recent years, research has also reported the emergence and spread of important antibiotic-resistant K. pneumoniae isolates across different regions of Iran (7,8). According to Shadkam et al, antibiotic resistance in biofilm-producing K. pneumoniae strains is a significant issue, as it limits treatment options in hospital settings. Their study highlights the need for basic measures and innovative strategies to manage biofilm-related infections in Iran (9). In addition to antibiotic resistance, which is a major problem in K. pneumoniae infections, the virulence and pathogenicity of K. pneumoniae strains are also important. Virulence genes in K. pneumoniae contribute significantly to disease progression, and understanding these genes is essential for understanding highly virulent and resistant strains. In addition, genes responsible for bacterial capsule formation are crucial in determining the capsule’s antigenic type, which differentiates isolates according to their pathogenic properties (2).
In addition to these cases, important pathotypes or resistant strains of K. pneumoniae can be identified through genotype analysis of the isolates. Assessing clonal relatedness among K. pneumoniae isolates is essential for designing effective infection control strategies. Molecular typing techniques such as enterobacterial repetitive intergenic consensus polymerase chain reaction (ERIC-PCR), are valuable tools for genetic typing and comparing genetic variability among strains (10,11). Regarding hospital-acquired infections, genetic profiling of K. pneumoniae from various hospital sites provides insights into genetic diversity, transmission patterns, and epidemiological patterns. Determining the relatedness among isolates helps track strains, detect outbreaks, and implement infection control measures. In this regard, the present study aimed to enhance understanding of K. pneumoniae epidemiology by examining antibiotic resistance status, the presence of resistance and capsular virulence genes, and genetic variability among isolates obtained from different hospital departments.
Materials and Methods
Sampling, Ethics, and Study Population
Sampling was conducted during the summer and autumn of 2023 using clinical specimens, including urine, blood, respiratory sputum, vaginal swabs, abscess drainage, and wound exudates. The samples were collected from 15 different hospital units in Amol, Mazandaran province, northern Iran, including outpatients (n = 418), surgery (n = 98), intensive care units (ICU) (n = 88), infectious (n = 59), emergency (n = 55), internal (n = 45), obstetrics and gynecology (n = 28), dialysis (n = 27), inpatients, (n = 23), pediatric (n = 13), neurology (n = 10), ear, nose, and throat (ENT) (n = 4), oncology (n = 2), coronary care unit (n = 1), and urology (n = 1).
A total of 872 samples (536 from female patients and 336 from male patients) were tested for the presence of K. pneumonia. Among these, 661 samples were obtained for urine culture (UC), 114 for sputum culture (SC), 68 for wound culture (WC), 18 for abscess discharge culture (AC), 8 for vaginal culture (VC), and 3 for blood culture (BC). Participants were classified into eight age groups: infant (0-2 years), child (2-12 years), adolescent (12-19 years), young adult (19-24 years), adult (24-44 years), middle-aged (44-65 years), elderly (65-80 years), and above 80 years (12).
Ethical approval for this study was obtained from the Ethics Committee of Amol University of Special Modern Technologies (Ethics Code: IR.AUSMT.1403.03). Furthermore, this study adhered to the ethical principles outlined in the Declaration of Helsinki. Informed consent was obtained from all participants or guardians of children. Written consent confirmed voluntary participation and a clear understanding of the study’s objectives, methodology, and associated risks. Participants were assured that their personal information would be used only for research purposes, with guaranteed protection of privacy and confidentiality throughout the study.
Cultivation Assay and Identification of Klebsiella pneumoniae
For the identification of K. pneumoniae, samples were incubated at 37 °C for 48 hours on blood agar and MacConkey agar. Lactose-fermenting mucoid colonies were subjected to Gram staining. Identification of isolates was based on colony appearance, morphology, and routine biochemical tests. These tests included indole, Voges-Proskauer/methyl red, Simmons citrate, lysine, ornithine decarboxylation, lactose fermentation, gas production, urease activity, O-nitrophenyl-D-glucopyranoside (ONPG) utilization, potassium cyanide (KCN) tolerance, catalase and oxidase production, and motility (13). Other bacteria were identified to the genus level using Gram staining, catalase and oxidase tests, bacterial movement assessment, oxidative-fermentative (O-F) tests, and other relevant biochemical assays. Isolates were maintained in brain heart infusion (BHI) broth supplemented with 20% (v/v) glycerol at -20 °C and preserved in the culture collection of the Bacteriology Laboratory at Amol University of Special Modern Technologies, Amol, Iran. K. pneumoniae (ATCC 700603) and Escherichia coli (ATCC 25922) were used as reference strains for antibiotic susceptibility testing, as well as for other bacteriological and genotyping assays.
Antibiotic Susceptibility Testing
According to the Clinical and Laboratory Standards Institute (CLSI) criteria (14), antimicrobial susceptibility testing was performed using the Mueller-Hinton agar (HiMedia, India) disk diffusion test. Sixteen antibiotics from 10 different classes were tested using antibiotic disks supplied by Padtan Teb, Iran. The antibiotic classes and their respective agents included:
Glycylcyclines: tetracycline (TE, 30 μg)
Cephalosporins: ceftazidime (CAZ, 30 μg), ceftriaxone (CRO, 30 μg), cefazolin (CZ, 30 μg), cephalexin (CP, 30 μg)
Folate pathway inhibitors: trimethoprim\sulfamethoxazole (SXT, 1.25/23.75 μg),
Aminoglycosides: gentamicin (GM, 10 μg), amikacin (AN, 30 μg)
Fluoroquinolones: ciprofloxacin (CIP, 5 μg),
Phosphonic acid derivatives: fosfomycin (FM, 50 μg)
Macrolides: erythromycin (E, 15 μg)
Carbapenems: imipenem (IPM,10 μg), meropenem (MEN, 10 μg), ertapenem (ETP, 10 μg),
Penicillins: ampicillin (AM,10 μg), monobactams: aztreonam (AZM, 30 μg).
Muller Hinton agar plates were incubated at 35 ± 2 °C for 18 hours, and then the diameters of the inhibition zones were recorded and compared to reference values provided by CLSI. Minimal inhibitory concentration (MIC) of colistin (Polymyxin E, CST) for the isolates was determined using the broth microdilution technique following the European Committee on Antimicrobial Susceptibility Testing (EUCAST) guidelines (15). K. pneumoniae isolates with an MIC > 2 mg/L were considered resistant to CST. The results were interpreted according to the CLSI guidelines. CRKP was defined, based on CLSI standards (14), as any isolate resistant to one or more carbapenem drugs, including IPM, ETP, or MEN. Furthermore, isolates were categorized based on the European Center for Disease Prevention and Control (ECDC) as follows:
-
MDR: isolates resistant to three or more antimicrobial classes;
-
Extremely drug-resistant (XDR): isolates alarmingly resistant to all, or nearly all, licensed antimicrobial agents;
-
Pan drug-resistant (PDR): isolates resistant to all antibiotic classes (14).
Extended-Spectrum β-Lactamases Isolates
An extended-spectrum β-lactamase (ESBL) positive test was conducted employing the Double Disc Synergy Test (DDST), using CAZ discs (30 µg), CAZ-clavulanate discs (30 µg/10 µg), cefotaxime (CTX) discs (30 µg), and CTX-clavulanate discs (30 µg/10 µg). A positive result was defined as an increase of ≥ 5 mm in the inhibition zone surrounding the CTX- or CAZ-clavulanate disc compared to the disc without clavulanate (16). K. pneumoniae (ATCC 700603) and E. coli (ATCC 25922) were used as reference strains for quality control.
DNA Extraction
DNA was extracted using a Gram-negative DNA purification kit (Sinaclon, Tehran, Iran) according to the manufacturer’s guidelines. DNA concentrations were initially measured using a BioSpectrometer (Eppendorf, Germany), and samples were subsequently normalized based on their concentration. Purified DNA samples were kept at -20 °C for application in the subsequent steps of the study.
Detection of Resistance Genes
The isolates were subjected to testing to identify the presence of 13 resistance genes, including aac (responsible for GM resistance), blaCTX-M-15, blaTEM-1A, blaVEB, and blaSHV (responsible for β-lactamases), tetA, tetB, and tetC (tetracycline resistance), sul1 and sul2 (sulfonamide resistance), dfrA1 (trimethoprim resistance), ereA (erythromycin resistance), and qnrA (quinolone resistance), and mcr (CST resistance). The primers used for amplification are listed in Table 1 (17-27). Standard PCR reactions were performed in a final volume of 25 μL, consisting of 12.5 µL of PCR master mix (Sinaclon, Iran), 0.5 μM of each reverse and forward primer, and 2 µL of DNA per sample. Finally, PCR products were analyzed by electrophoresis on a 1.5% agarose gel using a 100 bp marker (Sinaclon, Iran) for confirmation. Distinct resistance gene patterns were identified based on their occurrence.
Table 1.
Nucleotide Sequences of Primers Used in PCR for the Identification of Resistance Genes and Capsular Types in K. pneumoniae Isolates
|
Target Gene
|
Sequence (5' to 3')
|
Annealing Temperature (°C)
|
PCR Product Size (bp)
|
Reference
|
|
aac (3)
|
F: CTTCAGGATGGCAAGTTGGT
R: TCATCTCGTTCTCCGCTCAT |
55 |
286 |
(17) |
|
blaCTX-M-15
|
F: CATGTGCAGYACCAGTAA
R: CCGCRATATCRTTGGTGGTG |
42 |
542 |
(18) |
|
blaTEM-1A
|
F: ATGAGTATTCAACATTTCCG
R: CCAATGCTTAATCAGTGAGG |
46 |
850 |
(19) |
|
blaVEB-19
|
F: CGACTTCCATTTCCCGATGC
R: GGACTCTGCAACAAATACGC |
51 |
643 |
(20) |
|
blaSHV
|
F: TCGCCTGTGTATTATCTCCC
R: CGCAGATAAATCACCACAATG |
52 |
768 |
(20) |
|
tetA
|
F: GCTACATCCTGCTTGCCTTC
R: CATAGATCGCCGTGAAGAGG |
50 |
210 |
(21) |
|
tetB
|
F: TTGGTTAGGGGCAAGTTTTG
R: GTAATGGGCCAATAACACCG |
50 |
659 |
(22) |
|
tetC
|
F: CCTCTTGCGGGATATCGTCC
R: GGTTGAAGGCTCTCAAGGGC |
55 |
505 |
(23) |
|
sul1
|
F: TTCGGCATTCTGAATCTCAC
R: ATGATCTAACCCTCGGTCTC |
47 |
822 |
(24) |
|
sul2
|
F: CGGCATCGTCAACATAACC
R: GTGTGCGGATGAAGTCAG |
51 |
720 |
(24) |
|
ereA
|
F: GCCGGTGCTCATGAACTTGAG
R: CGACTCTATTCGATCAGAGGC |
52 |
419 |
(17) |
|
dfrA1
|
F: GGAGTGCCAAAGGTGAACAGC
R: GAGGCGAAGTCTTGGGTAAAAAC |
45 |
367 |
(25) |
|
qnrA
|
F: ATTTCTCACGCCAGGATTTG
R: GATCGGCAAAGGTTAGGTCA |
50 |
516 |
(26) |
|
mcr
|
F: CGGTCAGTCCGTTTGTTC
R: CTTGGTCGGTCTGTAGGG |
51 |
309 |
(27) |
|
WzyK1
|
F: GGTGCTCTTTACATCATTGC
R: GCAATGGCCATTTGCGTTAG |
52 |
1283 |
(28) |
|
WzyK2
|
F: GACCCGATATTCATACTTGACAGAG
R: CCTGAAGTAAAATCGTAAATAGATGGC |
52 |
641 |
(28) |
|
WzyK3
|
F: TAGGCAATTGACTTTAGGTG
R: AGTGAATCAGCCTTCACCT |
52 |
549 |
(28) |
|
WzyK5
|
F: TGGTAGTGATGCTCGCGA
R: CCTGAACCCACCCCAATC |
52 |
280 |
(28) |
|
WzyK20
|
F: CGGTGCTACAGTGCATCATT
R: GTTATACGATGCTCAGTCGC |
52 |
741 |
(28) |
|
WzyK54
|
F: CATTAGCTC AGT GGT TGG CT
R: GCTTGACAAACACCATAGCAG |
52 |
881 |
(28) |
|
WzyK57
|
F: CTCAGGGCTAGAAGTGTCAT
R: CACTAACCCAGAAAGTCGAG |
52 |
1037 |
(28) |
Note. PCR: Polymerase chain reaction; K. pneumoniae: Klebsiella pneumoniae; F: Forward; R: Reverse.
Identification of Hypervirulent Klebsiella pneumoniae and Capsular Type
Single-round PCR assays were used for molecular typing of the K. pneumoniae capsular types. Specific PCR reactions were conducted to amplify the capsular genes wzyK1, wzyK2, wzyK3, wzyK5, wzyK20, wzyK54, and wzyK57 using their respective primers, as depicted in Table 1 (28,29). A string test was used for every isolate as an initial screening method for identifying hypervirulent K. pneumoniae (hvKP). Hyperviscosity was also confirmed by observing the formation of a mucoviscous cord exceeding 5 mm when an inoculation loop was utilized to pass through a colony cultured on agar medium (30).
Enterobacterial Repetitive Intergenic Consensus Polymerase Chain Reaction DNA Fingerprinting
The ERIC-PCR was utilized to assess the genotypic profiles of the isolates. Each reaction mixture was prepared in a total volume of 25 μL, comprising 1.5 μL of each primer at a final concentration of 2 pmol/μL, 12.5 μL of Master Mix (SinnaClon, Iran), and 8.5 μL of deionized distilled water. The ERIC-PCR utilized primer ERIC-1 (5’-ATGTAAGCTCCTGGGGATTCAC-3’) and primer ERIC-2 (5’-AAGTAAGTGACTGGGGTGAGCG-3’), following the previously established protocol (31). Subsequently, GelClust software was used to analyze the images obtained from the ERIC-PCR results (32). Genetic similarities among the isolates were determined using the Pearson correlation coefficient, applying a 2% optimization tolerance and a 4% positional tolerance shift. In addition, a dendrogram was constructed based on the Dice correlation coefficient, employing the unweighted pair group method with arithmetic averages (UPGMA).
Statistical Analysis
To identify potential correlations among the various variables, statistical analysis was carried out using SPSS version 23 (IBM, Armonk, North Castle, NY, USA). The Mann–Whitney, chi-square, and Kolmogorov–Smirnov tests were employed for data analysis. The significance level was set at a P value of < 0.05.
Results
Distribution of Klebsiella pneumoniae in Hospitalized Patients
Klebsiella pneumoniae was isolated from 70 samples (8.02%) out of a total of 872 clinical specimens collected and cultured from different hospital units. Among the samples collected, E. coli, Pseudomonas aeruginosa, Citrobacter, and Listeria were isolated in 163 (18.69%), 78 (8.94%), 14 (1.6%), and 2 (0.22%) samples, respectively. A total of 524 samples showed no microbial growth. Seventy K. pneumoniae isolates were obtained from various clinical samples, including 41/661 from urine (6.2%), 18/114 from sputum (15.7%), six from abscesses (33.33%), three from blood (100%), and two from wound specimens (2.9%). Among the 15 hospital units evaluated, K. pneumoniae was not isolated from any samples collected from the obstetrics and gynecology, oncology, or ENT units. Statistical analysis revealed no significant association between patient hospitalization and the presence of K. pneumoniae (P ≥ 0.05). Additionally, positive isolates were observed in 41 of 536 (7.64%) female samples and 29 of 336 (8.63%) male samples, which was not statistically significant (P ≥ 0.05). However, a substantial relationship was found between the sampling site and K. pneumoniae isolation (P ≤ 0.05).
Antibiotic Susceptibility, Extended-Spectrum β-Lactamase, and Carbapenem-Resistant Klebsiella pneumoniae Isolates
Antibiotic resistance results of K. pneumoniae isolates are summarized in Table 2. The highest resistance rates were observed for erythromycin (98.6%), AM (92.9%), and CZ (68.6%). Notably, none of the isolates exhibited resistance to CST. Of the 70 isolates, 39 (55.71%) and 11 (15.71%) isolates of K. pneumoniae were detected as MDR and XDR, respectively, while no isolates were detected as PDR. Among all K. pneumoniae isolates, 31 (44.28%) were identified as ESBL, and CRKP was observed in 39 (55.71%) of the isolates. Statistical analysis indicated a significant relationship between AM resistance and samples from the ICU, infectious diseases, internal medicine, and outpatient units (P ≤ 0.05). Furthermore, resistance to CZ, fosfomycin, and erythromycin showed a significant relationship with isolates from infectious diseases and the ICU units (P ≤ 0.05). Resistance to GM, FM, and CZ antibiotics was significantly higher in isolates obtained from sputum samples (P ≤ 0.05). However, no significant relationship was identified between resistance to specific antibiotics and patient gender or age group. Similarly, no significant correlations were observed between the presence of ESBL and CRKP isolates and the other investigated variables (e.g., age group, hospital unit, sample type, ERIC-PCR pattern, hvKP, and capsular type). In addition, no significant association was observed between MDR and XDR isolates and other investigated variables.
Table 2.
Antibiotic Resistance Among Klebsiella pneumoniae Isolated From Hospitals
|
Antibiotic
|
Number of Isolates (%)
|
|
Susceptible
|
Intermediate
|
Resistant
|
| TE |
48 (68.8) |
10 (14.3) |
12 (17.1) |
| CAZ |
21 (30) |
5 (7.1) |
44 (62.9) |
| CRO |
26 (37.1) |
2 (2.9) |
42 (60) |
| CZ |
17 (24.3) |
5 (7.1) |
48 (68.6) |
| CP |
18 (25.7) |
10 (14.3) |
42 (60) |
| SXT |
32 (45.7) |
3 (4.3) |
35 (50) |
| GM |
26 (37.1) |
10 (14.3) |
34 (48.6) |
| AN |
14 (20) |
20 (28.6) |
36 (51.4) |
| CIP |
33 (47.1) |
- |
37 (52.9) |
| FM |
31 (44.3) |
6 (8.6) |
33 (47.1) |
| E |
1 (1.4) |
- |
69 (98.6) |
| IPM |
21 (30) |
11 (15.7) |
38 (54.3) |
| MEN |
26 (37.1) |
10 (14.3) |
34 (48.6) |
| ETP |
21 (30) |
11 (15.7) |
38 (54.3) |
| AM |
3 (4.3) |
2 (2.9) |
65 (92.9) |
| CST |
70 (100) |
- |
- |
| AZM |
18 (25.7) |
14 (20) |
38 (54.3) |
Note. TE: Tetracycline, CAZ: Ceftazidime; CRO: Ceftriaxone; CZ: Cefazolin, CP: Cephalexin; SXT: Trimethoprim\sulfamethoxazole; GM: Gentamicin; AN: Amikacin; CIP: Ciprofloxacin; FM: Fosfomycin (FM), E: erythromycin; IPM: Imipenem; MEN: Meropenem; ETP: Ertapenem; AM: Ampicillin; CST: Colistin; AZM: Aztreonam.
Results of Resistance Gene Detection
Table 3 displays detailed information regarding the detection of the resistance-related genes in K. pneumoniae isolates. The tetB gene was detected among all 70 isolates. The mcr and the blaVEB genes were not identified in any of the isolates. The blaSHV and the sul1 genes showed a substantial relation with isolates obtained from male patients (P ≤ 0.05). Additionally, the tetA gene demonstrated a significant relation with isolates from patients aged 65 to 80 years (P ≤ 0.05). In total, 48 different resistance gene patterns were identified across the 70 isolates (Table 4). The tetB / dfrA /sul1/ blatTEM pattern was the most common observed pattern with a frequency of 6 (8.57%).
Table 3.
Distribution of Resistance Genes Among ERIC-PCR Phylogenetic Groups of Klebsiella pneumoniae
|
Phylogenetic Group
|
No
|
Resistance Gene Distribution (%)
|
Total
Genes
|
|
Sul1
|
Sul2
|
qnr
|
dfrA
|
ereA
|
aac
|
tetA
|
tetB
|
tetC
|
blaTEM
|
blaVEB
|
blaCTX-M
|
blaSHV
|
mcr
|
14
|
| E-1 |
3 |
2 |
1 |
0 |
0 |
0 |
1 |
1 |
3 |
0 |
0 |
0 |
0 |
0 |
0 |
5 |
| E-2 |
9 |
6 |
0 |
1 |
5 |
0 |
3 |
5 |
9 |
0 |
3 |
0 |
2 |
3 |
0 |
9 |
| E-3 |
7 |
4 |
0 |
0 |
4 |
0 |
0 |
3 |
7 |
0 |
3 |
0 |
1 |
2 |
0 |
7 |
| E-4 |
2 |
0 |
1 |
0 |
0 |
0 |
1 |
0 |
2 |
0 |
0 |
0 |
0 |
1 |
0 |
4 |
| E-5 |
1 |
0 |
0 |
0 |
0 |
0 |
0 |
1 |
1 |
0 |
1 |
0 |
1 |
0 |
0 |
4 |
| E-6 |
1 |
1 |
0 |
0 |
1 |
0 |
0 |
0 |
1 |
0 |
1 |
0 |
0 |
0 |
0 |
4 |
| E-7 |
3 |
2 |
1 |
0 |
1 |
0 |
0 |
0 |
3 |
1 |
1 |
0 |
0 |
1 |
0 |
7 |
| E-8 |
2 |
2 |
0 |
0 |
2 |
0 |
0 |
0 |
2 |
1 |
2 |
0 |
0 |
1 |
0 |
6 |
| E-9 |
1 |
0 |
0 |
0 |
0 |
0 |
0 |
0 |
1 |
0 |
0 |
0 |
0 |
0 |
0 |
1 |
| E-10 |
2 |
2 |
2 |
0 |
0 |
0 |
0 |
0 |
2 |
0 |
1 |
0 |
0 |
0 |
0 |
4 |
| E-11 |
2 |
2 |
0 |
0 |
0 |
0 |
2 |
0 |
2 |
0 |
1 |
0 |
0 |
0 |
0 |
4 |
| E-12 |
1 |
0 |
0 |
0 |
0 |
0 |
0 |
0 |
1 |
0 |
1 |
0 |
1 |
1 |
0 |
4 |
| E-13 |
1 |
0 |
0 |
0 |
0 |
1 |
0 |
0 |
1 |
0 |
0 |
0 |
0 |
0 |
0 |
2 |
| E-14 |
1 |
1 |
0 |
0 |
1 |
0 |
1 |
0 |
1 |
1 |
0 |
0 |
0 |
0 |
0 |
5 |
| E-15 |
8 |
4 |
2 |
0 |
3 |
0 |
0 |
2 |
8 |
0 |
4 |
0 |
1 |
4 |
0 |
8 |
| E-16 |
1 |
0 |
0 |
0 |
1 |
0 |
0 |
1 |
1 |
0 |
1 |
0 |
0 |
0 |
0 |
4 |
| E-17 |
1 |
1 |
0 |
0 |
0 |
0 |
0 |
0 |
1 |
0 |
0 |
0 |
0 |
1 |
0 |
3 |
| E-18 |
2 |
0 |
0 |
0 |
0 |
2 |
0 |
1 |
2 |
1 |
2 |
0 |
0 |
1 |
0 |
6 |
| E-19 |
1 |
0 |
0 |
0 |
0 |
0 |
0 |
0 |
1 |
0 |
1 |
0 |
0 |
1 |
0 |
3 |
| E-20 |
1 |
1 |
0 |
0 |
0 |
0 |
0 |
0 |
1 |
0 |
0 |
0 |
0 |
0 |
0 |
2 |
| E-21 |
2 |
1 |
1 |
0 |
1 |
0 |
0 |
1 |
2 |
0 |
1 |
0 |
0 |
1 |
0 |
7 |
| E-22 |
1 |
0 |
0 |
0 |
0 |
0 |
1 |
0 |
1 |
0 |
1 |
0 |
0 |
0 |
0 |
3 |
| E-23 |
15 |
10 |
1 |
0 |
10 |
0 |
4 |
5 |
15 |
0 |
10 |
0 |
2 |
5 |
0 |
9 |
| E-24 |
2 |
1 |
0 |
0 |
1 |
0 |
1 |
0 |
2 |
0 |
1 |
0 |
0 |
0 |
0 |
5 |
| Total |
|
40
(57.14) |
9
(12.85) |
1
(1.42) |
30
(42.85) |
3
(4.28) |
14
(20) |
20
(28.57) |
70
(100) |
4
(5.71) |
35
(50) |
0
(0) |
8
(11.42) |
22
(31.42) |
0
(0) |
- |
Note. ERIC-PCR: Intergenic consensus-polymerase chain reaction.
Table 4.
Resistance Gene Patterns of the Klebsiella pneumoniae Isolates Recovered From Hospital Units
|
Number of Genes
|
Resistance Gene Pattern
|
Number of Isolates (%)
|
Source
|
Hospital Unit
|
| 1 |
tetB
|
4 (5.71) |
UC, SC |
Outpatients, ICU |
| 2 |
tetA / tetB
|
2 (2.85) |
BC, UC |
Dialysis, Outpatients |
|
tetB / ereA
|
1 (1.42) |
UC |
Outpatients |
|
tetB /sul1
|
1 (1.42) |
UC |
Internal |
|
tetB /sul2
|
2 (2.85) |
UC |
Internal |
|
tetB / blaTEM
|
3 (4.28) |
AC, SC, WC |
Infectious, ICU, Urology |
| 3 |
tetA / tetB / blaTEM
|
1 (1.42) |
UC |
Internal |
|
tetA / tetB / blaSHV
|
1 (1.42) |
AC |
Infectious |
|
tetA / tetB /sul1
|
1 (1.42) |
UC |
Outpatients |
|
tetB / aac / dfrA
|
1 (1.42) |
SC |
Inpatients |
|
tetB / dfrA /sul1
|
4 (5.71) |
SC, UC |
ICU, Infectious, Internal |
|
tetB / aac / blaTEM
|
2 (2.85) |
SC |
ICU |
|
tetB / tetC /sul2
|
1 (1.42) |
UC |
Outpatients |
|
tetB / qnr / blaTEM
|
1 (1.42) |
UC |
Outpatients |
|
tetB / blaSHV
/sul1
|
2 (2.85) |
SC, UC |
Internal, Outpatients |
|
tetB / blaSHV
/ blaTEM
|
4 (5.71) |
UC |
Internal, Outpatients, Infectious |
|
tetB / aac /sul1
|
1 (1.42) |
BC |
Dialysis |
|
tetB /sul1/sul2
|
1 (1.42) |
UC |
Outpatients |
| 4 |
tetA / tetB / aac /sul1
|
1 (1.42) |
UC |
Outpatients |
|
tetA / tetB / dfrA /sul1
|
1 (1.42) |
SC |
ICU |
|
tetA / tetB / dfrA / blaTEM
|
1 (1.42) |
UC |
ICU |
|
tetA / tetB / blaCTX-M
/ blaTEM
|
1 (1.42) |
UC |
ICU |
|
tetA / tetB / blaCTX-M
/ blaSHV
|
1 (1.42) |
UC |
Outpatients |
|
tetA / tetB / blaCTX-M
/ dfrA
|
1 (1.42) |
UC |
Outpatients |
|
tetB / ereA / blaSHV
/ blaTEM
|
1 (1.42) |
UC |
Outpatients |
|
tetB / aac /sul1/ blaTEM
|
1 (1.42) |
UC |
Outpatients |
|
tetB / aac /sul1/sul2
|
1 (1.42) |
UC |
Outpatients |
|
tetB / blaCTX-M
/ blaSHV
/ blaTEM
|
1 (1.42) |
UC |
Surgery |
|
tetB / dfrA / blaSHV
/sul1
|
1 (1.42) |
UC |
Emergency |
|
tetB / blaSHV
/sul2/ blaTEM
|
1 (1.42) |
SC |
ICU |
|
tetB /sul1/sul2/ blaTEM
|
1 (1.42) |
UC |
Outpatients |
|
tetB / dfrA /sul1/ bla
TEM
|
6 (8.57) |
SC, BC, UC |
ICU, Dialysis, Pediatrics, CCU, Outpatients |
|
tetB / aac / dfrA /sul1
|
1 (1.42) |
AC |
Infectious |
|
tetB / aac / bla
SHV
/sul2
|
1 (1.42) |
AC |
Infectious |
|
tetB / bla
CTX-M
/ dfrA /sul1
|
1 (1.42) |
SC |
ICU |
| 5 |
tetA / tetB / bla
SHV
/sul1/ bla
TEM
|
1 (1.42) |
SC |
ICU |
|
tetA / tetB / aac / dfrA /sul1
|
1 (1.42) |
UC |
Outpatients |
|
tetA / tetB / tetC / ereA / bla
TEM
|
1 (1.42) |
UC |
Outpatients |
|
tetA / tetB / dfrA /sul1/ bla
TEM
|
1 (1.42) |
UC |
Outpatients |
|
tetB / tetC / aac / dfrA /sul1
|
1 (1.42) |
WC |
Surgery |
|
tetB / tetC / dfrA /sul1/ bla
TEM
|
1 (1.42) |
UC |
Outpatients |
|
tetB / dfrA / bla
SHV
/sul1/ bla
TEM
|
2 (2.85) |
SC |
Neurology, ICU |
|
tetA / tetB / bla
SHV
/sul2/ bla
TEM
|
1 (1.42) |
AC |
Infectious |
| 6 |
tetA / tetB / dfrA / bla
SHV
/sul1/ bla
TEM
|
2 (2.85) |
UC |
Outpatients |
|
tetB / aac / bla
CTX-M
/ dfrA / bla
SHV
/sul1
|
1 (1.42) |
UC |
Outpatients |
|
tetA / tetB / aac / dfrA /sul1/ bla
TEM
|
1 (1.42) |
SC |
ICU |
|
tetB / bla
CTX-M
/ dfrA / bla
SHV
/sul1/ bla
TEM
|
1 (1.42) |
AC |
Infectious |
| 7 |
tetA / tetB / aac / dfrA / bla
SHV
/sul1/ bla
TEM
|
1 (1.42) |
SC |
ICU |
| Total |
48 |
70 |
5 |
12 |
Note. ICU: Intensive care unit; CCU: Coronary care unit.
Capsular Genes and Hypervirulent Klebsiella pneumoniae Identification
Among the 70 isolates analyzed, 44 (62.85%) isolates were identified as hvKP. Capsular typing revealed that 52 isolates (74.28%) belonged to type K57, while 3 isolates (4.28%) were identified as type K54, totaling 55 capsular-typed isolates. The capsular types of 15 isolates (21.42%) were not recognized, and capsular types K1, K2, K3, K5, and K20 were not identified in any of the isolates. A statistically significant correlation was detected between hvKP isolates and the presence of the K57 capsular type (P ≤ 0.05). Furthermore, there was a significant relationship between the occurrence of the dfrA and blaSHV resistance genes and the K57 capsular type (P ≤ 0.05). However, the K57 capsular type did not show a significant relationship with ERIC-PCR genotypic patterns, patient age group, sex, hospitalization variables, or resistance-specific antibiotics (P ≥ 0.05).
Results of DNA Fingerprinting
The results of ERIC-PCR DNA fingerprinting analysis for the isolates are presented in Figure 1, which includes a dendrogram along with information on resistance gene patterns, sample types, hospital units, and capsular types for each isolate. A total of 24 separate clusters were identified using ERIC-PCR analysis via GelClust (UPGMA), labeled E-1 to E-24, with a discriminatory power of 0.9159 and Simpson’s Index of Diversity (SID) of 0.08406. A notable relationship was observed between the presence of ereA and tetC resistance genes and specific ERIC-PCR clusters (P < 0.05). However, no significant associations were found between ERIC-PCR genotypes and the patients’ age or gender, the hospital unit, or the sample type from which K. pneumoniae was isolated (P > 0.05). Among the studied antibiotics, a significant correlation was observed between resistance to CAZ and ERIC-PCR genotypes (P < 0.05).
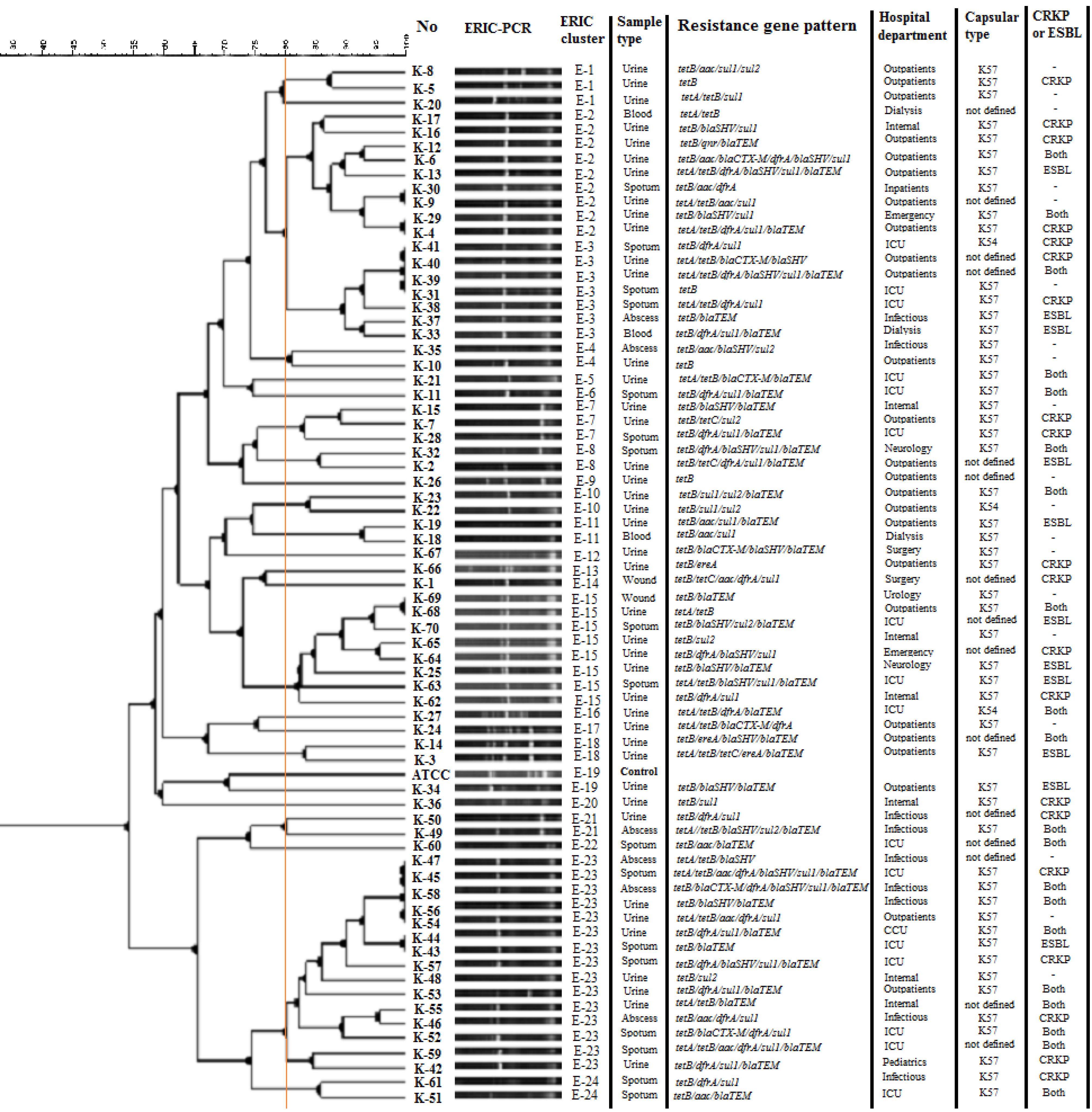
Figure 1.
Dendrogram based on ERIC-PCR fingerprinting of K. pnumoniae isolates using the UPGMA analysis, in associated with resistance gene pattern, hospital unit, and sample and capsular type
.
Dendrogram based on ERIC-PCR fingerprinting of K. pnumoniae isolates using the UPGMA analysis, in associated with resistance gene pattern, hospital unit, and sample and capsular type
Discussion
Various studies highlight the importance of addressing the spread of pathogens such as K. pneumoniae, underscoring the need for monitoring antimicrobial resistance trends and implementing effective infection control practices to prevent the spread of resistant strains and improve patient outcomes (9,33). The present study, conducted in northern Iran, revealed a high prevalence of K. pneumoniae in clinical samples collected from hospitalized patients. The research focused on the association between sampling sites and K. pneumoniae isolation rates, calling for targeted surveillance. Recent studies across different regions of Iran have demonstrated the emergence of resistant K. pneumoniae strains, with a particular focus on carbapenem-resistant isolates. However, most of these studies have been limited in scope, particularly regarding the assessment of bacterial prevalence and diversity across different hospital departments (34).
The present study indicated widespread antibiotic resistance among K. pneumoniae isolates, especially against erythromycin, AM, and CZ, highlighting the need for judicious use of antibiotics. Different perspectives can be debated with research in various countries and regions. For example, research conducted in the United States reported extensive antimicrobial resistance in K. pneumoniae isolates, especially against nitrofurantoin and trimethoprim/sulfamethoxazole (35). The prevalence of ESBL-positive and antibiotic non-susceptible strains showed geographical and age-related variability, with a general trend of increasing resistance over time. These significant variations in resistance patterns highlight the need for tailored treatment strategies that consider regional and demographic differences.
Studies conducted in Iran and Poland also emphasized the considerable challenge of managing antimicrobial resistance in K. pneumoniae strains, underscoring the critical need for ongoing surveillance and effective intervention measures (8,36). A previous study in Iran reported that CST-resistant K. pneumoniae isolates harbored the mcr gene (7), but this resistance gene was not detected in the present study. Notably, 20 isolates (28.57%) were found to be both ESBL producers and CRKP simultaneously.
Several studies have reported the prevalence and clinical importance of resistance genes in K. pneumoniae. Elbadawi et al in Sudan identified the blaCTX-M as the most prevalent resistance gene among carbapenem-resistant Gram-negative bacilli, contributing to hospital-acquired infections (5). Likewise, Li et al in China reported an increasing trend in the presence of blaCTX-M and blaSHV genes in hvKP strains, emphasizing their association with virulence and resistance traits (30). Further, a study by Manandhar et al in Nepal identified sul1, sul2, blaTEM and blaCTX-M genes in MDR strains in hospital settings (6).
These findings collectively illustrate the extensive genetic diversity of resistance determinants in K. pneumoniae, reflecting their significant role in antimicrobial resistance surveillance and control worldwide. This study revealed that tetB, sul1, and blaTEM were the most prevalent genes within their respective antibiotic groups. Among 70 isolates, 48 distinct plasmid-borne resistance gene patterns reflected significant genetic diversity and resistance variations in hospital settings.
Capsular genes considerably affect the pathogenicity of K. pneumoniae. The gene clusters responsible for capsular polysaccharide production, particularly the Wzy and Wzx genes involved in polymerization and assembly, are pivotal for CPS subunit formation. The sequence diversity of the Wzy gene is crucial for the development of PCR-based capsular typing assays (37). In the present study, WzyK57 was the predominant capsular gene, showing a significant association with hypervirulent strains, as well as with the dfrA and blaSHV resistance genes. In contrast, WzyK54 was detected in only three isolates. No substantial associations were found between the dominant capsular type and hospital unit, sample type, patient age, or patient sex. Furthermore, other known capsular-related genes were absent in the K. pneumoniae isolates analyzed. These findings contrast with previous studies, which have reported different prevalent capsular types (37,38).
In this study, ERIC-PCR was used for genotyping isolates from various hospital wards. Molecular typing using ERIC-PCR established distinct clusters of isolates, with specific genotypes demonstrating specific resistance gene profiles and antibiotic susceptibility patterns. Notably, genotypes E-2 and E-23 had the highest number of resistance genes, whereas E-9 had only two. Although the ERIC-PCR genotypes exhibited no significant relationship with other studied variables, all 70 K. pneumoniae isolates were successfully typed using this method. The diversity and number of observed genotypes indicate that ERIC-PCR provided adequate discriminatory power for molecular typing. Recent studies have highlighted the high discriminatory power of ERIC-PCR, equivalent to PFGE, for K. pneumoniae typing. Kundu et al demonstrated ERIC-PCR’s superiority over MALDI-TOF MS in detecting clonal relationships among MDR K. pneumoniae strains (11).
In conclusion, this study underscores ERIC-PCR’s ability to elucidate genotype-antimicrobial resistance relationships. However; there was no evidence to suggest this method is effective for identifying MDR strains. In a similar study, Abed et al used ERIC-PCR to identify 23 distinct ERIC types among 15 MDR K. pneumoniae isolates, indicating considerable genetic diversity and a polyclonal nature within hospital settings (10). In addition, ERIC-PCR showed rapid, reliable, and cost-effective performance compared to other methods, making it a valuable tool for assessing genetic diversity and clonal relationships among MDR K. pneumoniae isolates in Egypt (13).
Conclusion
The study highlights the prevalence of MDR and CRKP isolates in specific hospital units and sample types in Amol, northern Iran. The K57 capsular type was the most prevalent among hvKP isolates recovered from medical centers in the region. Among all K. pneumoniae isolates analyzed, tetB, sul1, and blaTEM were the most commonly detected resistance genes, corresponding to their respective antibiotic groups. The application of ERIC-PCR genotyping enabled the identification of genetic clusters associated with certain resistance genes and antibiotic resistance profiles, shedding light on the genotypic variation of K. pneumoniae strains in the hospital setting. These findings support the need for the implementation of targeted antimicrobial stewardship programs that emphasize strict infection control measures in high-risk areas such as ICUs and surgical wards. Surveillance for MDR and CRKP strains should be conducted routinely, with a focus on identifying specific resistance profiles and capsular typing to guide appropriate antibiotic therapy. Moreover, the identification of prevalent resistance genes, including tetB, sul1, and blaTEM, underscores the importance of ongoing monitoring of these genes in clinical settings. We recommend further research into the underlying genetic mechanisms of resistance, which will contribute to the development of more effective treatment strategies and inform hospital-level guidelines for infection prevention and control.
Acknowledgments
This study was supported by the Islamic Azad University, Ayatollah Amoli branch, and Amol University of Special Modern Technologies, Amol, Iran. We thank all staff members of the Department of Pathobiology at Amol University of Special Modern Technologies for their cooperation and invaluable support throughout the research period. Special thanks are due to F. Mahdavi for her technical assistance.
Competing Interests
None declared.
Funding
None.
References
- Diab H, Rahy K, Jisr T, El Chaar M, Abboud E, Tokajian S. Phenotypic and molecular characterization of multi-drug resistant Klebsiella spp isolates recovered from clinical settings. Infect Genet Evol 2024; 119:105583. doi: 10.1016/j.meegid.2024.105583 [Crossref] [ Google Scholar]
- Zakaria SB, Gad GF, Mahmoud MA, Elfarash AE, Elmokhtar MA, Mohamed HA. Resistance profiles, virulence factors, genotypes and clinical outcomes of Klebsiella pneumonia isolated from patients with community-acquired pneumonia. Afro-Egypt J Infect Enem Dis 2024;14(2):154-72. doI: 10.21608/aeji.2024.267386.1355.
- Sid Ahmed MA, Hamid JM, Hassan AMM, Abu Jarir S, Bashir Ibrahim E, Abdel Hadi H. Phenotypic and genotypic characterization of pan-drug-resistant Klebsiella pneumoniae isolated in Qatar. Antibiotics (Basel) 2024; 13(3):275. doi: 10.3390/antibiotics13030275 [Crossref] [ Google Scholar]
- Jian X, Li Y, Wang H, Li C, Li F, Li J. A comparative study of genotyping and antimicrobial resistance between carbapenem-resistant Klebsiella pneumoniae and Acinetobacter baumannii isolates at a tertiary pediatric hospital in China. Front Cell Infect Microbiol 2024; 14:1298202. doi: 10.3389/fcimb.2024.1298202 [Crossref] [ Google Scholar]
- Elbadawi HS, Elhag KM, Mahgoub E, Altayb HN, Ntoumi F, Elton L. Detection and characterization of carbapenem resistant gram-negative bacilli isolates recovered from hospitalized patients at Soba University Hospital, Sudan. BMC Microbiol 2021; 21(1):136. doi: 10.1186/s12866-021-02133-1 [Crossref] [ Google Scholar]
- Manandhar S, Zellweger RM, Maharjan N, Dongol S, Prajapati KG, Thwaites G. A high prevalence of multi-drug resistant gram-negative bacilli in a Nepali tertiary care hospital and associated widespread distribution of extended-spectrum beta-lactamase (ESBL) and carbapenemase-encoding genes. Ann Clin Microbiol Antimicrob 2020; 19(1):48. doi: 10.1186/s12941-020-00390-y [Crossref] [ Google Scholar]
- Moosavian M, Emam N. The first report of emerging mobilized colistin-resistance (mcr) genes and ERIC-PCR typing in Escherichia coli and Klebsiella pneumoniae clinical isolates in southwest Iran. Infect Drug Resist 2019; 12:1001-10. doi: 10.2147/idr.S192597 [Crossref] [ Google Scholar]
- Heidary M, Nasiri MJ, Dabiri H, Tarashi S. Prevalence of drug-resistant Klebsiella pneumoniae in Iran: a review article. Iran J Public Health 2018; 47(3):317-26. [ Google Scholar]
- Shadkam S, Goli HR, Mirzaei B, Gholami M, Ahanjan M. Correlation between antimicrobial resistance and biofilm formation capability among Klebsiella pneumoniae strains isolated from hospitalized patients in Iran. Ann Clin Microbiol Antimicrob 2021; 20(1):13. doi: 10.1186/s12941-021-00418-x [Crossref] [ Google Scholar]
- Abed NS, Kariptas E, Lateef SA. Molecular typing of MDR-K pneumoniae using ERIC-PCR technique. Res J Pharm Technol 2022; 15(10):4677-80. doi: 10.52711/0974-360x.2022.00784 [Crossref] [ Google Scholar]
- Kundu J, Kansal S, Rathore S, Kaundal M, Angrup A, Biswal M. Evaluation of ERIC-PCR and MALDI-TOF as typing tools for multidrug resistant Klebsiella pneumoniae clinical isolates from a tertiary care center in India. PLoS One 2022; 17(11):e0271652. doi: 10.1371/journal.pone.0271652 [Crossref] [ Google Scholar]
- Geifman N, Cohen R, Rubin E. Redefining meaningful age groups in the context of disease. Age (Dordr) 2013; 35(6):2357-66. doi: 10.1007/s11357-013-9510-6 [Crossref] [ Google Scholar]
- Baraka K, Abozahra R, Haggag MM, Abdelhamid SM. Genotyping and molecular investigation of plasmid-mediated carbapenem resistant clinical Klebsiella pneumoniae isolates in Egypt. AIMS Microbiol 2023; 9(2):228-44. doi: 10.3934/microbiol.2023014 [Crossref] [ Google Scholar]
- Clinical and Laboratory Standards Institute (CLSI). Performance Standards for Antimicrobial Susceptibility Testing. 32th ed. CLSI Supplement M100. Wayne, PA: CLSI; 2022.
- European Committee on Antimicrobial Susceptibility Testing. Breakpoint tables for Interpretation of MICs and Zone Diameters, Version 60. 2020. Available from: http://www.eucast.org.
- Sajeev S, Hamza M, Rajan V, Vijayan A, Sivaraman GK, Shome BR. Resistance profiles and genotyping of extended-spectrum beta-lactamase (ESBL) - producing and non-ESBL-producing E coli and Klebsiella from retail market fishes. Infect Genet Evol 2023; 112:105446. doi: 10.1016/j.meegid.2023.105446 [Crossref] [ Google Scholar]
- Van TT, Chin J, Chapman T, Tran LT, Coloe PJ. Safety of raw meat and shellfish in Vietnam: an analysis of Escherichia coli isolations for antibiotic resistance and virulence genes. Int J Food Microbiol 2008; 124(3):217-23. doi: 10.1016/j.ijfoodmicro.2008.03.029 [Crossref] [ Google Scholar]
- Saladin M, Cao VT, Lambert T, Donay JL, Herrmann JL, Ould-Hocine Z. Diversity of CTX-M beta-lactamases and their promoter regions from Enterobacteriaceae isolated in three Parisian hospitals. FEMS Microbiol Lett 2002; 209(2):161-8. doi: 10.1111/j.1574-6968.2002.tb11126.x [Crossref] [ Google Scholar]
- Eckert C, Gautier V, Arlet G. DNA sequence analysis of the genetic environment of various blaCTX-M genes. J Antimicrob Chemother 2006; 57(1):14-23. doi: 10.1093/jac/dki398 [Crossref] [ Google Scholar]
- Naas T, Mikami Y, Imai T, Poirel L, Nordmann P. Characterization of In53, a class 1 plasmid- and composite transposon-located integron of Escherichia coli which carries an unusual array of gene cassettes. J Bacteriol 2001; 183(1):235-49. doi: 10.1128/jb.183.1.235-249.2001 [Crossref] [ Google Scholar]
- Faldynova M, Pravcova M, Sisak F, Havlickova H, Kolackova I, Cizek A. Evolution of antibiotic resistance in Salmonella enterica serovar typhimurium strains isolated in the Czech Republic between 1984 and 2002. Antimicrob Agents Chemother 2003; 47(6):2002-5. doi: 10.1128/aac.47.6.2002-2005.2003 [Crossref] [ Google Scholar]
- Levings RS, Partridge SR, Lightfoot D, Hall RM, Djordjevic SP. New integron-associated gene cassette encoding a 3-N-aminoglycoside acetyltransferase. Antimicrob Agents Chemother 2005; 49(3):1238-41. doi: 10.1128/aac.49.3.1238-1241.2005 [Crossref] [ Google Scholar]
- Sengeløv G, Agersø Y, Halling-Sørensen B, Baloda SB, Andersen JS, Jensen LB. Bacterial antibiotic resistance levels in Danish farmland as a result of treatment with pig manure slurry. Environ Int 2003; 28(7):587-95. doi: 10.1016/s0160-4120(02)00084-3 [Crossref] [ Google Scholar]
- Maynard C, Fairbrother JM, Bekal S, Sanschagrin F, Levesque RC, Brousseau R. Antimicrobial resistance genes in enterotoxigenic Escherichia coli O149:K91 isolates obtained over a 23-year period from pigs. Antimicrob Agents Chemother 2003; 47(10):3214-21. doi: 10.1128/aac.47.10.3214-3221.2003 [Crossref] [ Google Scholar]
- Toro CS, Farfán M, Contreras I, Flores O, Navarro N, Mora GC. Genetic analysis of antibiotic-resistance determinants in multidrug-resistant Shigella strains isolated from Chilean children. Epidemiol Infect 2005; 133(1):81-6. doi: 10.1017/s0950268804003048 [Crossref] [ Google Scholar]
- Shams E, Firoozeh F, Moniri R, Zibaei M. Prevalence of plasmid-mediated quinolone resistance genes among extended-spectrum β-lactamase-producing Klebsiella pneumoniae human isolates in Iran. J Pathog 2015; 2015:434391. doi: 10.1155/2015/434391 [Crossref] [ Google Scholar]
- Liu YY, Wang Y, Walsh TR, Yi LX, Zhang R, Spencer J. Emergence of plasmid-mediated colistin resistance mechanism MCR-1 in animals and human beings in China: a microbiological and molecular biological study. Lancet Infect Dis 2016; 16(2):161-8. doi: 10.1016/s1473-3099(15)00424-7 [Crossref] [ Google Scholar]
- Ssekatawa K, Byarugaba DK, Nakavuma JL, Kato CD, Ejobi F, Tweyongyere R. Prevalence of pathogenic Klebsiella pneumoniae based on PCR capsular typing harbouring carbapenemases encoding genes in Uganda tertiary hospitals. Antimicrob Resist Infect Control 2021; 10(1):57. doi: 10.1186/s13756-021-00923-w [Crossref] [ Google Scholar]
- Zhang S, Yang G, Ye Q, Wu Q, Zhang J, Huang Y. Phenotypic and genotypic characterization of Klebsiella pneumoniae isolated from retail foods in China. Front Microbiol 2018; 9:289. doi: 10.3389/fmicb.2018.00289 [Crossref] [ Google Scholar]
- Li W, Sun G, Yu Y, Li N, Chen M, Jin R. Increasing occurrence of antimicrobial-resistant hypervirulent (hypermucoviscous) Klebsiella pneumoniae isolates in China. Clin Infect Dis 2014; 58(2):225-32. doi: 10.1093/cid/cit675 [Crossref] [ Google Scholar]
- Versalovic J, Koeuth T, Lupski JR. Distribution of repetitive DNA sequences in eubacteria and application to fingerprinting of bacterial genomes. Nucleic Acids Res 1991; 19(24):6823-31. doi: 10.1093/nar/19.24.6823 [Crossref] [ Google Scholar]
- Khakabimamaghani S, Najafi A, Ranjbar R, Raam M. GelClust: a software tool for gel electrophoresis images analysis and dendrogram generation. Comput Methods Programs Biomed 2013; 111(2):512-8. doi: 10.1016/j.cmpb.2013.04.013 [Crossref] [ Google Scholar]
- Parrott AM, Shi J, Aaron J, Green DA, Whittier S, Wu F. Detection of multiple hypervirulent Klebsiella pneumoniae strains in a New York City hospital through screening of virulence genes. Clin Microbiol Infect 2021; 27(4):583-9. doi: 10.1016/j.cmi.2020.05.012 [Crossref] [ Google Scholar]
- Zahedi Bialvaei A, Eslami P, Ganji L, Dolatyar Dehkharghani A, Asgari F, Koupahi H. Prevalence and epidemiological investigation of mgrB-dependent colistin resistance in extensively drug resistant Klebsiella pneumoniae in Iran. Sci Rep 2023; 13(1):10680. doi: 10.1038/s41598-023-37845-z [Crossref] [ Google Scholar]
- Kaye KS, Gupta V, Mulgirigama A, Joshi AV, Ye G, Scangarella-Oman NE. Prevalence, regional distribution, and trends of antimicrobial resistance among female outpatients with urine Klebsiella spp isolates: a multicenter evaluation in the United States between 2011 and 2019. Antimicrob Resist Infect Control 2024; 13(1):21. doi: 10.1186/s13756-024-01372-x [Crossref] [ Google Scholar]
- Kot B, Piechota M, Szweda P, Mitrus J, Wicha J, Grużewska A. Virulence analysis and antibiotic resistance of Klebsiella pneumoniae isolates from hospitalised patients in Poland. Sci Rep 2023; 13(1):4448. doi: 10.1038/s41598-023-31086-w [Crossref] [ Google Scholar]
- Taha MS, Hagras MM, Shalaby MM, Zamzam YA, Elkolaly RM, Abdelwahab MA. Genotypic characterization of carbapenem-resistant Klebsiella pneumoniae isolated from an Egyptian University Hospital. Pathogens 2023; 12(1):121. doi: 10.3390/pathogens12010121 [Crossref] [ Google Scholar]
- Choi M, Hegerle N, Nkeze J, Sen S, Jamindar S, Nasrin S. The diversity of lipopolysaccharide (O) and capsular polysaccharide (K) antigens of invasive Klebsiella pneumoniae in a multi-country collection. Front Microbiol 2020; 11:1249. doi: 10.3389/fmicb.2020.01249 [Crossref] [ Google Scholar]