Avicenna Journal of Clinical Microbiology and Infection. 12(2):61-66.
doi: 10.34172/ajcmi.3605
Original Article
Prevalence of Erythromycin Resistance Genes in Gram-Positive and Gram-Negative Bacteria From Secondary Infections
Mohammadsaid Golabi Data curation, Formal analysis, Investigation, Software, Visualization, Writing – original draft, 1 
Maryam Mohammadi-Sichani Conceptualization, Funding acquisition, Methodology, Project administration, Resources, Supervision, Writing – review & editing, 1, *
Sodabeh Rostami Conceptualization, Data curation, Methodology, Validation, 2
Author information:
1Department of Microbiology, Fal.C., Faculty of Biological Science, Islamic Azad University, Isfahan, Iran
2Infectious Diseases and Tropical Medicine Research Center, Isfahan University of Medical Sciences, Isfahan, Iran
Abstract
Background: Bacterial secondary infections in patients can exacerbate disease symptoms and significantly increase mortality rates. This study aimed to evaluate the prevalence of bacterial agents responsible for secondary infections in hospitalized patients and to identify the presence of erythromycin resistance genes (ermB, ermA, and mefA) in bacterial isolates.
Methods: Samples from secondary infections were collected from hospitalized patients to determine the most prevalent bacterial pathogens and assess their resistance profiles using the polymerase chain reaction method.
Results: The bacterial species most frequently associated with secondary infections were Escherichia coli (32.2%), Klebsiella pneumoniae (31.2%), Enterococcus faecalis (24.3%), and Acinetobacter baumannii (11.3%). Testing for antibiotic susceptibility indicated that most bacterial isolates were resistant to erythromycin and ciprofloxacin. Notably, the ermB gene was detected in 89.6% of the isolates, while ermA and mefA genes were absent in all bacterial isolates.
Conclusion: These findings underscore the significant level of erythromycin resistance among pathogens responsible for secondary infections in hospitalized patients, with a predominant association with the ermB gene. This highlights the pressing need for improved antibiotic stewardship and the development of alternative therapeutic strategies to combat the growing threat of secondary bacterial infections in clinical settings.
Keywords: Secondary infections, Erythromycin, Resistance genes, ermB protein, Multidrug-resistant
Copyright and License Information
© 2025 The Author(s); Published by Hamadan University of Medical Sciences.
This is an open-access article distributed under the terms of the Creative Commons Attribution License (
https://creativecommons.org/licenses/by/4.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Please cite this article as follows: Golabi M, Mohammadi-Sichani M, Rostami S. Prevalence of erythromycin resistance genes in gram-positive and gram-negative bacteria from secondary infections. Avicenna J Clin Microbiol Infect. 2025;12(2):61-66. doi:10.34172/ajcmi.3605
Introduction
Erythromycin, a macrolide antibiotic, has long been a cornerstone in the treatment of bacterial infections, particularly those caused by gram-positive organisms, such as Streptococcus and Staphylococcus species. However, resistance to erythromycin has also emerged among gram-negative bacilli, raising significant concerns for infection control and public health (1).
Erythromycin is a macrolide antibiotic that inhibits bacterial protein synthesis by binding to the 50S ribosomal subunit. This action is more effective against gram-positive bacteria because their ribosomes are more accessible. However, gram-negative bacteria have an outer membrane that can restrict erythromycin’s entry, thus making them less susceptible. Gram-negative bacilli exhibit resistance to erythromycin primarily through efflux systems that actively pump the antibiotic out of the cell, thereby preventing its accumulation. These systems, often encoded by genes such as mef (A), significantly lower the intracellular concentration of erythromycin, rendering it ineffective. Although this mechanism is more common in gram-positive bacteria, certain gram-negative bacilli can also acquire resistance through the methylation of ribosomal RNA by erm (erythromycin ribosome methylase) genes. This methylation reduces erythromycin’s binding affinity to the 23S ribosomal RNA in bacterial ribosomes, further diminishing its efficacy (2).
The spread of erythromycin resistance among gram-negative bacilli presents a significant challenge in the treatment of bacterial infections. This resistance not only limits the effectiveness of erythromycin and related macrolides but often necessitates the use of alternative antibiotics. The problem is particularly acute in hospital settings, where resistant bacteria are more prevalent (3).
Despite the introduction of newer antibiotics that have reduced mortality rates associated with secondary infections, the overall incidence of such infections remains high. Moreover, the overuse of antibiotics has contributed to the emergence and spread of resistant bacterial strains, further complicating treatment efforts (4,5). Secondary infections have led to substantial human and financial losses worldwide in recent years. Secondary infection occurs when a new infection develops following a primary infection, often due to a weakened immune system, tissue damage, or disrupted microbiota. Preventive measures include vaccination, proper antibiotic use, and good hygiene maintenance to reduce the risk of complications. The availability of clinical data on bacterial infections is essential for guiding effective treatment strategies and mitigating the impact of these infections (6). This study aims to investigate the bacterial agents associated with secondary infections and evaluate the prevalence of erythromycin resistance genes among these pathogens.
Materials and Methods
Bacterial Strain
This study was conducted on 100 samples collected from patients with secondary infections hospitalized in medical centers in Isfahan in 2023. The specimens were cultured on Eosin-Methylene Blue agar and blood agar. Bacterial colonies were assessed for phenotypic characteristics, followed by Gram staining and biochemical tests to identify bacterial isolates.
The Kirby-Bauer disk diffusion method was employed to evaluate the antimicrobial susceptibility profiles of the isolates to commonly used antibiotics. Antibiotic discs containing erythromycin (15 µg), azithromycin (5 µg), penicillin G (10 µg), vancomycin (30 µg), ciprofloxacin (5 µg), gentamicin (10 µg), tetracycline (30 µg), and linezolid (10 µg) were placed on Mueller-Hinton agar plates inoculated with the isolates. The diameters of the inhibition zones around the discs were compared against the Clinical and Laboratory Standards Institute (CLSI) guidelines. Based on these standards, the isolates were categorized as resistant, intermediate, or susceptible (7).
Minimum Inhibitory Concentration and Minimum Bactericidal Concentration Determination
Erythromycin MIC was determined using a microdilution approach in 96-well microtiter plates. The amount of antibiotic required to prepare the stock solution was calculated based on CLSI guidelines using the following formula:
Weight of powder (mg) = [volume of solution (mL) × concentration (µg/mL)] / [potency of powder (µg/mg)]
The MIC was defined as the lowest concentration of the antibiotic at which no turbidity was observed, indicating the inhibition of visible bacterial growth. To determine the MBC, aliquots from wells without visible growth were subcultured onto fresh agar plates. The MBC was identified as the lowest antibiotic concentration that achieved a 99.9% reduction in the initial bacterial count. The results were then compared with the standard reference values provided by the CLSI (8).
Molecular Identification of Selected Isolates
Target genes (ermA, ermB, and mefA) were identified via polymerase chain reaction (PCR) amplification using gene-specific primers listed in Table 1 (9,10). Genomic DNA was obtained through a heat-based extraction protocol.
Table 1.
The Specifications of Primers Used for Erythromycin Resistance Genes
|
Product Length (bp)
|
Nucleotide Sequence
|
Gene Name
|
| 189 |
5'-AAGCGGTAAACCCCTCTGA-3' |
ermA
|
| 5'-TTCGCAAATCCCTTCTCAAC-3' |
| 424 |
5'-GGAACATCTGTGGTATGGCG-3' |
ermB
|
| 5'-CAT TTAACGACGAAACTGGC-3' |
| 348 |
5'-AGTATCATTAATCACTAGTGC-3' |
mefA
|
| 5'-TTCTTCTGGTACTAAAAGTGG-3' |
The PCR mixture consisted of 25 µL, including 0.25 µL (1.25 U/µL) of Taq DNA polymerase, 0.5 µL (0.25 mM) of deoxynucleotide triphosphates (dNTPs), 0.75 µL (1.5 mM) of MgCl₂, 1 µL (5 pmol/µL) of forward and reverse primers, 17 µL of double-distilled water, and 2.0 µL of template DNA. PCR was initiated with a denaturation step at 94 °C for 3 minutes, followed by 30 cycles comprising denaturation (94 °C for 30 seconds), annealing (55 °C for 30 seconds), and extension (72 °C for 45 seconds). A final elongation was performed at 72 °C for 5 minutes. Amplification products were resolved by electrophoresis on a 1.5% agarose gel and visualized using SYBR Green fluorescence (11).
Data Analysis
Data processing and statistical evaluation were conducted using SPSS (version 21), and a P-value less than 0.05 was considered indicative of a significant difference.
Results
The study included 100 samples from patients with secondary infections, of which 66.0% were female and 34.0% were male. The frequency of secondary infections was significantly higher in females than in males, as determined by the chi-square test (P= 0.001). The age of the patients with secondary infections ranged from 1 year to 96 years, with an average age of 59.38 ± 23.94 years (Table 2). The highest frequency of secondary infections was observed in the age group of 60–79 years (34.0%). Based on the chi-square test, a significant difference in infection frequency was found across different age groups (P < 0.001). However, Fisher’s exact test did not reveal a significant difference in infection frequency between males and females.
Table 2.
Antibiotic Resistance Patterns Among Isolates From Secondary Infections
|
Antibiotic
|
E. coli
|
K. pneumoniae
|
E. faecalis
|
A.
baumannii
|
P
Value
|
|
No.
|
%
|
No.
|
%
|
No.
|
%
|
No.
|
%
|
| Erythromycin |
34 |
91.9a |
34 |
94.4a |
25 |
89.3a |
8 |
57.1b |
0.021 |
| Azithromycin |
26 |
70.3 a |
27 |
75.0 a |
25 |
89.3 b |
6 |
42.8 c |
0.064 |
| Vancomycin |
- |
- |
- |
- |
16 |
57.1 b |
- |
- |
0.086 |
| Ampicillin |
35 |
94.6 a |
33 |
91.7 a |
17 |
60.7 b |
14 |
100.0 a |
0.063 |
| Ciprofloxacin |
31 |
83.8a |
31 |
86.1 a |
18 |
64.3b |
14 |
100.0 c |
0.032 |
| Tetracycline |
35 |
94.6 a |
33 |
91.7 a |
22 |
78.6 b |
14 |
100.0 a |
0.508 |
| Gentamycin |
30 |
81.1 a |
33 |
91.7 a |
20 |
71.4 b |
13 |
92.9 a |
0.891 |
Note. E. coli: Escherichia coli; K. pneumoniae: Klebsiella pneumoniae; E. faecalis: Enterococcus faecalis; A. baumannii: Acinetobacter baumannii. *Numbers marked in a row with the same letters had no significant difference in terms of antibiotic resistance.
A total of 115 bacterial isolates were recovered from 100 samples of secondary infections. One bacterial isolate was obtained from each of the 85 samples, while two isolates were obtained from each of the remaining 15 samples. The identified isolates included 37, 36, 14, and 28 Escherichia coli, Klebsiella pneumoniae, Acinetobacter baumannii, and Enterococcus faecalis, respectively (Figure 1).
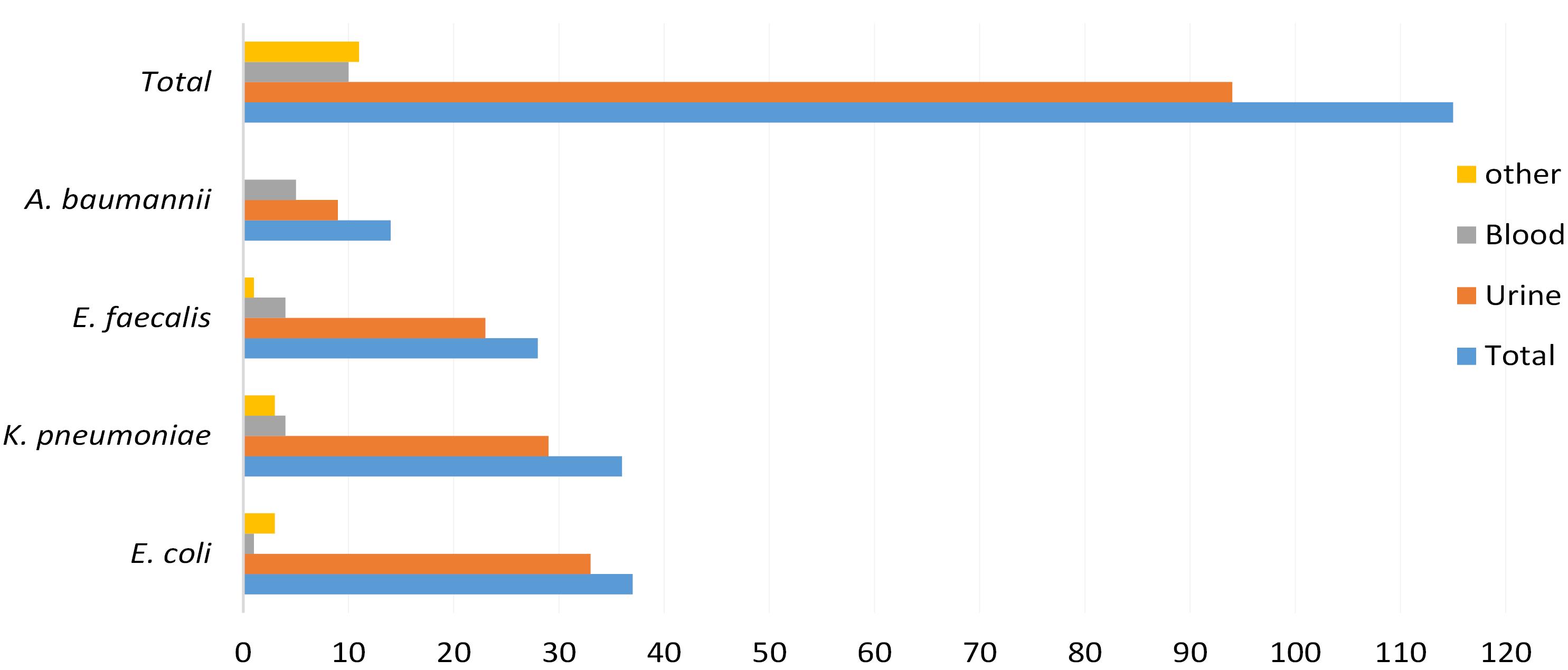
Figure 1.
Distribution of Bacteria Isolated From Secondary Infections. Note. E. coli: Escherichia coli; K. pneumoniae: Klebsiella pneumoniae; E. faecalis: Enterococcus faecalis; A. baumannii: Acinetobacter baumannii
.
Distribution of Bacteria Isolated From Secondary Infections. Note. E. coli: Escherichia coli; K. pneumoniae: Klebsiella pneumoniae; E. faecalis: Enterococcus faecalis; A. baumannii: Acinetobacter baumannii
The highest prevalence of secondary infections was observed in urinary tract infections (UTIs) (81.7%), followed by blood infections (8.7%). On the other hand, the lowest prevalence was associated with joint fluid, peritoneal fluid, cerebrospinal fluid, wound cultures, and tracheal tube samples (Table 1). Fisher’s exact test revealed no significant relationship between the type of infection and the type of bacterial isolate (P = 0.096).
Based on the results of the antibiotic susceptibility testing, all bacterial isolates were resistant to at least one antibiotic. The highest resistance was found against erythromycin (89.6%), followed by ciprofloxacin (62.1%) and gentamycin (75.0%). Interestingly, resistance to azithromycin was observed in 70.3% of the isolates. Significant differences in resistance were noted for erythromycin, ciprofloxacin, and linezolid among the bacterial isolates. In terms of antibiotic resistance profiles, E. coli isolates were more sensitive to antibiotics compared to other isolates, whereas A. baumannii isolates exhibited the lowest sensitivity to antibiotics (Table 2).
The MIC values of erythromycin for isolates in the susceptibility test were determined using the broth microdilution method (Table 3). The frequency of erythromycin-resistant bacteria ranged from 16.4% in E. coli to 90.9% in A. baumannii, as determined by the microdilution plate method.
Table 3.
MIC Values of Erythromycin for 115 Isolates
|
Bacteria
|
MIC (µg/mL)
|
|
>0.2
|
>0.4
|
>0.8
|
>0.16
|
>0.32
|
>0.64
|
>0.128
|
>0.256
|
>0.512
|
|
E. faecalis
|
- |
- |
- |
2 |
- |
1 |
2 |
13 |
10 |
|
E. coli
|
1 |
- |
3 |
1 |
3 |
3 |
4 |
15 |
7 |
|
K. pneumoniae
|
1 |
- |
1 |
1 |
3 |
1 |
4 |
18 |
7 |
|
A. baumannii
|
2 |
1 |
- |
1 |
1 |
3 |
- |
2 |
3 |
Note. MIC: Minimum inhibitory concentration; E. coli: Escherichia coli; K. pneumoniae: Klebsiella pneumoniae; E. faecalis: Enterococcus faecalis; A. baumannii: Acinetobacter baumannii.
An investigation into the presence of erythromycin resistance genes in the isolates revealed that ermB was the most detected gene in E. coli, K. pneumoniae, E. faecalis, and A. baumannii (Figure 2).
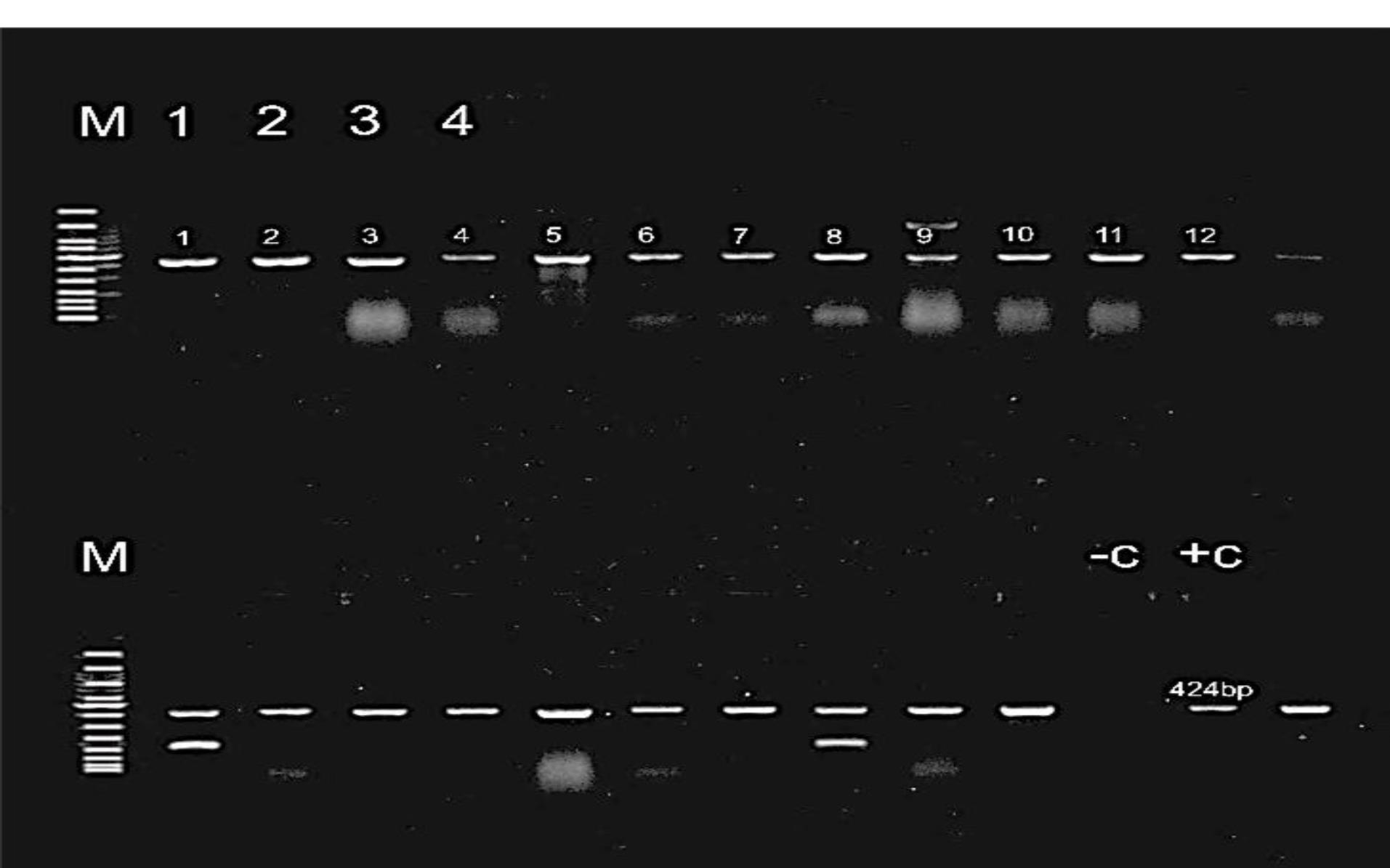
Figure 2.
Agarose Gel Electrophoresis of the ermB Gene. Note. S. aureus: Staphylococcus aureus. A S. aureus strain with ermB and distilled water were the positive control (C + ) and the negative control (C), respectively. Bands corresponding to the ermB gene are observed at 424 bp
.
Agarose Gel Electrophoresis of the ermB Gene. Note. S. aureus: Staphylococcus aureus. A S. aureus strain with ermB and distilled water were the positive control (C + ) and the negative control (C), respectively. Bands corresponding to the ermB gene are observed at 424 bp
The ermA and mefA genes were not observed in any of the isolates. Additionally, the relationship between the presence of the ermB gene and resistance to erythromycin and azithromycin was examined, and no significant association was found in E. coli and E. faecalis (Figure 3).
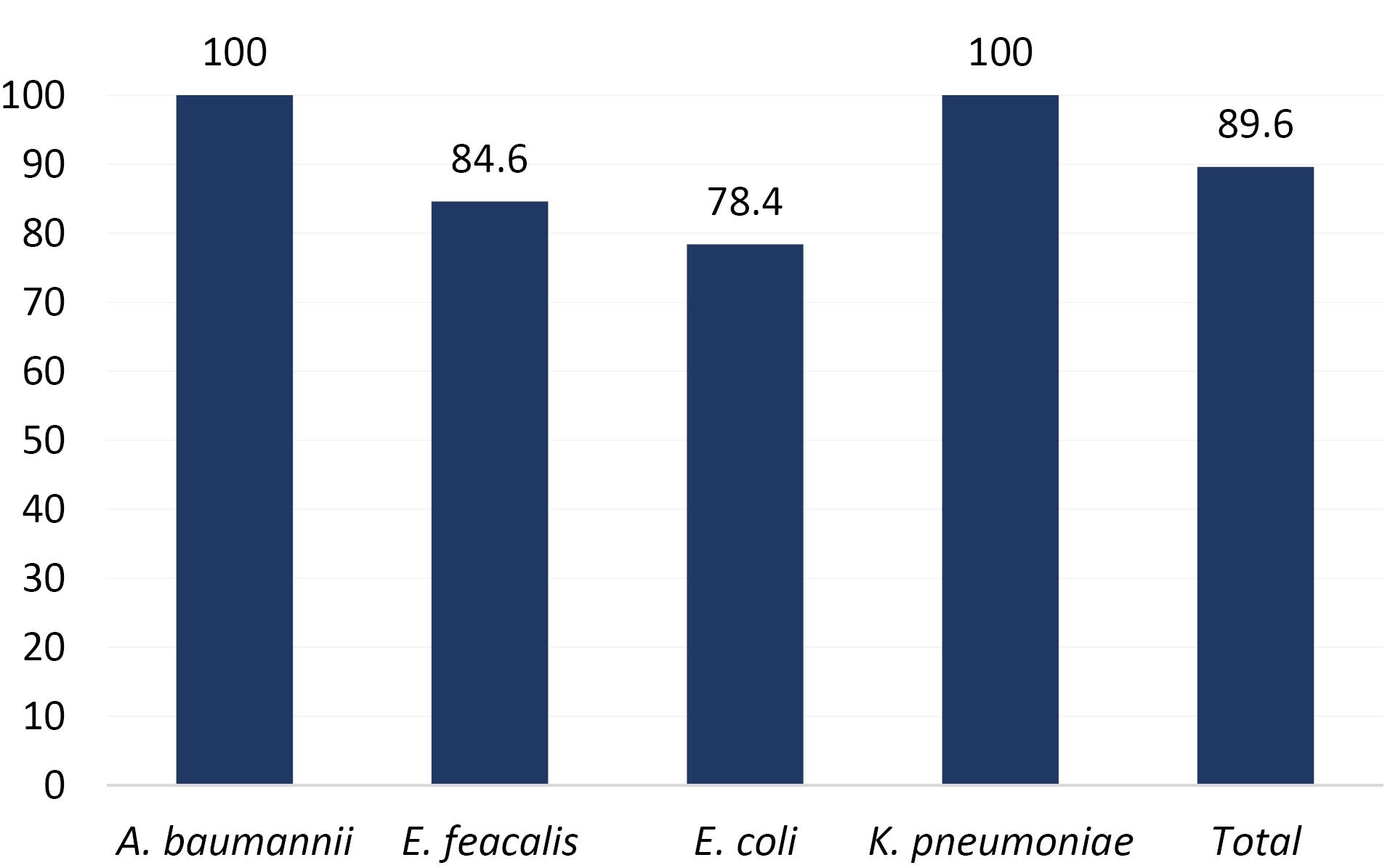
Figure 3.
Prevalence of the ermB Resistance Gene in Isolates From Secondary Infections. Note. E. coli: Escherichia coli; K. pneumoniae: Klebsiella pneumoniae; E. faecalis: Enterococcus faecalis; A. baumannii: Acinetobacter baumannii
.
Prevalence of the ermB Resistance Gene in Isolates From Secondary Infections. Note. E. coli: Escherichia coli; K. pneumoniae: Klebsiella pneumoniae; E. faecalis: Enterococcus faecalis; A. baumannii: Acinetobacter baumannii
Table 3 presents the relationship between the presence of the ermB gene and resistance to erythromycin and azithromycin in various isolates from secondary infections. According to the results of Fisher’s exact test, there was no significant association between erythromycin resistance and the presence of the ermB gene in E. coli (P= 0.343) and E. faecalis (P = 0.530).
The ermB gene was detected in all isolates of E. faecalis and A. baumannii. Based on the results of Fisher’s exact test (Table 4), no significant association was found between azithromycin resistance and the presence of the ermB gene in E. coli (P= 0.672) and E. faecalis (P = 0.408).
Table 4.
Association Between the Presence of the ermB Gene and Resistance to Azithromycin and Erythromycin in Secondary Infection Samples
|
Azithromycin
|
Erythromycin
|
|
Bacteria
|
Sensitive
|
Resistant
|
Carrying
ermB
|
P
Value
|
Sensitive
|
Resistant
|
Carrying
ermB
|
P
Value
|
|
%
|
No.
|
%
|
No.
|
|
%
|
No.
|
%
|
No.
|
|
|
E. coli
|
72.7 |
8 |
80.8 |
21 |
+ |
0.672 |
100.0 |
3 |
76.5 |
26 |
+ |
0.672 |
| 27.3 |
3 |
19.2 |
5 |
- |
0.0 |
0 |
23.5 |
8 |
- |
| 100.0 |
3 |
100.0 |
34 |
Total |
100.0 |
3 |
100.0 |
34 |
Total |
|
K. pneumoniae
|
100.0 |
9 |
100.0 |
27 |
+ |
- |
100.0 |
2 |
100.0 |
34 |
+ |
- |
| 0.0 |
0 |
0.0 |
0 |
- |
0.0 |
0 |
0.0 |
0 |
- |
| 100.0 |
9 |
100.0 |
27 |
Total |
100.0 |
2 |
100.0 |
34 |
Total |
|
E. faecalis
|
66.7 |
2 |
87.0 |
20 |
+ |
0.408 |
100.0 |
2 |
83.3 |
20 |
+ |
0.408 |
| 33.3 |
1 |
13.0 |
3 |
- |
0.0 |
0 |
16.7 |
4 |
- |
| 100.0 |
3 |
100.0 |
23 |
Total |
100.0 |
2 |
100.0 |
24 |
Total |
|
A. baumannii
|
100.0 |
7 |
100.0 |
6 |
+ |
- |
100.0 |
5 |
100.0 |
8 |
+ |
- |
| 0.0 |
0 |
0.0 |
0 |
- |
0.0 |
0 |
0.0 |
0 |
- |
| 100.0 |
7 |
100.0 |
6 |
Total |
|
|
|
|
Total |
Note. E. coli: Escherichia coli; K. pneumoniae: Klebsiella pneumoniae; E. faecalis: Enterococcus faecalis; A. baumannii: Acinetobacter baumannii.
Discussion
The present study identified E. coli, K. pneumoniae, and E. faecalis as the most common causes of secondary infections, with UTIs being the most frequent (81.7%). In addition, E. coli was the predominant pathogen in urinary infections, while A. baumannii was the most common cause of blood infections. Gram-negative bacilli, including K. pneumoniae and A. baumannii, were prevalent in secondary infections. In the study performed by Sharma et al on bacterial co-infections and secondary infections, A. baumannii and K. pneumoniae were the most common isolates (35.6% and 18.1%), respectively (12). Likewise, Saeed et al concluded that gram-negative (including K. pneumoniae, P. aeruginosa, multidrug-resistant A. baumannii, and E. coli) and Gram-positive (coagulase-negative Staphylococci, E. faecalis, E. faecium, and S. aureus) bacteria were the most common species (13).
The prevalence of secondary bacterial infections and the types of bacteria involved vary across studies and regions. While the current study and that of Saeed et al (13) found a high prevalence of gram-negative bacilli, studies conducted by Sharma et al (12) and Moreno-García et al reported different results in terms of the most common bacterial isolates (14). These variations may be due to regional bacterial strains, hospital settings, and patient populations. However, all studies emphasized the presence of drug-resistant bacteria, highlighting the importance of continuous monitoring and targeted antibiotic treatment strategies for patients with secondary bacterial infections.
Studies on erythromycin resistance in gram-negative bacilli indicate significant concerns regarding antibiotic resistance, especially from infections acquired in hospitals and the community. Resistance mechanisms in gram-negative bacteria often involve the production of efflux pumps, antibiotic-modifying enzymes, and alterations to the bacterial cell envelope, preventing effective penetration of antibiotics like erythromycin (15).
This study revealed the significant prevalence of the ermB gene in the bacterial isolates. However, the detection of the ermB gene did not show a direct association with azithromycin resistance in E. coli and E. faecalis, implying that other factors might play a role in the development of antibiotic resistance. These findings underscore the importance of continuously monitoring both antibiotic resistance patterns and the presence of resistance genes in bacterial infections.
Considering that erythromycin is not the preferred antibiotic for eliminating infections caused by gram-negative bacilli according to CLSI guidelines, there are limited published studies in this area (16). Nonetheless, given that erythromycin and azithromycin were used to treat secondary infections, they were considered in this study. The resistance levels to these two antibiotics were assessed in all gram-positive and gram-negative isolates. Rostami et al found that the ermTR and mefA genes were present in 37% and 11.1% of isolates, respectively (17). In the study by Akrami et al, the prevalence of secondary infections in southern Iran was reported as 72.7%, with S. aureus and K. pneumoniae being the most frequently isolated bacteria. Their findings also revealed that 68.7% of these isolates demonstrated multidrug resistance (18).
Based on the results of Fallah et al, erythromycin resistance in S. pneumoniae isolates was 84.93%. The ermB and mefA genes were identified in 58.06% and 16.13% of erythromycin-resistant S. pneumoniae, respectively (19). This is particularly concerning given the role of these bacteria in critical infections, including UTIs, respiratory tract infections, and infections associated with surgical wounds.
Roohbakhsh Ghiasi et al investigated the frequency of erythromycin resistance genes in Klebsiella, Enterobacter, and Proteus isolates from UTIs. The frequency of ermA and ermB genes in the 120 studied isolates was 22.5% and 20.6%, respectively, while phenotypic resistance to erythromycin was 76.7% (20). The high levels of resistance suggest that these bacteria may harbor multiple resistance mechanisms, such as the production of extended-spectrum beta-lactamases, which complicates treatment strategies. The presence of the ermB gene, which is linked to resistance to macrolides like erythromycin, has been frequently observed in various isolates. However, it is important to note that while the ermB gene may contribute to resistance, other genetic factors (e.g., modifications in antibiotic target sites or efflux pump activity) might also play a role in conferring resistance (21). Consequently, understanding these mechanisms is crucial for managing resistance in clinical settings, particularly as resistance continues to rise among gram-negative pathogens.
Conclusion
This study highlights the alarming prevalence of erythromycin resistance among bacterial pathogens associated with secondary infections in hospitalized patients, with the ermB gene emerging as the dominant resistance determinant. The detection of ermB in both gram-positive and gram-negative isolates, particularly in E. coli, K. pneumoniae, E. faecalis, and A. baumannii, underlines the gene’s potential role in widespread macrolide resistance. The absence of ermA and mefA suggests a localized genetic pattern of resistance that warrants further investigation. Our findings emphasize the urgent need for comprehensive antibiotic stewardship programs, continuous surveillance of resistance genes, and the development of novel antimicrobial therapies to mitigate the growing threat of multidrug-resistant infections in healthcare settings.
Competing Interests
The authors have no conflict of interests to declare.
Ethical Approval
This study was performed with the approval of the Medical Ethics Committee (ID: IR.IAU.PS.REC.1400.196). Informed consent for blood sampling and the bronchoalveolar lavage fluid procedure was obtained from each guardian.
Funding
This research was conducted with funding provided by the authors.
References
- Muteeb G, Rehman MT, Shahwan M, Aatif M. Origin of antibiotics and antibiotic resistance, and their impacts on drug development: a narrative review. Pharmaceuticals (Basel) 2023; 16(11):1615. doi: 10.3390/ph16111615 [Crossref] [ Google Scholar]
- Uddin TM, Chakraborty AJ, Khusro A, Zidan BR, Mitra S, Emran TB. Antibiotic resistance in microbes: History, mechanisms, therapeutic strategies and future prospects. J Infect Public Health 2021; 14(12):1750-66. doi: 10.1016/j.jiph.2021.10.020 [Crossref] [ Google Scholar]
- Sharma S, Chauhan A, Ranjan A, Mathkor DM, Haque S, Ramniwas S. Emerging challenges in antimicrobial resistance: implications for pathogenic microorganisms, novel antibiotics, and their impact on sustainability. Front Microbiol 2024; 15:1403168. doi: 10.3389/fmicb.2024.1403168 [Crossref] [ Google Scholar]
- Pompilio A, Pomponio S, Di Vincenzo V, Crocetta V, Nicoletti M, Piovano M. Antimicrobial and antibiofilm activity of secondary metabolites of lichens against methicillin-resistant Staphylococcus aureus strains from cystic fibrosis patients. Future Microbiol 2013; 8(2):281-92. doi: 10.2217/fmb.12.142 [Crossref] [ Google Scholar]
- Mahmoudi H. Bacterial co-infections and antibiotic resistance in patients with COVID-19. GMS Hyg Infect Control 2020; 15:Doc35. doi: 10.3205/dgkh000370 [Crossref] [ Google Scholar]
- Feldman C, Anderson R. The role of co-infections and secondary infections in patients with COVID-19. Pneumonia (Nathan) 2021; 13(1):5. doi: 10.1186/s41479-021-00083-w [Crossref] [ Google Scholar]
- Clinical and Laboratory Standards Institute (CLSI). Methods for Dilution Antimicrobial Susceptibility Tests for Bacteria That Grow Aerobically. 11th ed. CLSI; 2018.
- European Committee for Antimicrobial Susceptibility Testing (EUCAST) of the European Society of Clinical Microbiology and Infectious Diseases (ESCMID). Determination of minimum inhibitory concentrations (MICs) of antibacterial agents by broth dilution. Clin Microbiol Infect. 2003;9(8):ix-xv. doi: 10.1046/j.1469-0691.2003.00790.x.
- Dundar D, Sayan M, Tamer GS. Macrolide and tetracycline resistance and emm type distribution of Streptococcus pyogenes isolates recovered from Turkish patients. Microb Drug Resist 2010; 16(4):279-84. doi: 10.1089/mdr.2010.0021 [Crossref] [ Google Scholar]
- Timsina R, Shrestha U, Singh A, Timalsina B. Inducible clindamycin resistance and erm genes in Staphylococcus aureus in school children in Kathmandu, Nepal. Future Sci OA 2020; 7(1):FSO361. doi: 10.2144/fsoa-2020-0092 [Crossref] [ Google Scholar]
- Fazzeli H, Arabestani MR, Nasr Esfahani B, Khorvash F, Pourshafie MR, Moghim S. Development of PCR-based method for detection of Enterobacteriaceae in septicemia. J Res Med Sci 2012; 17(7):671-5. [ Google Scholar]
- Sharma B, Sreenivasan P, Biswal M, Mahajan V, Suri V, Singh Sehgal I. Bacterial coinfections and secondary infections in COVID-19 patients from a tertiary care hospital of northern India: time to adhere to culture-based practices. Qatar Med J 2021; 2021(3):62. doi: 10.5339/qmj.2021.62 [Crossref] [ Google Scholar]
- Saeed NK, Al-Khawaja S, Alsalman J, Almusawi S, Albalooshi NA, Al-Biltagi M. Bacterial co-infection in patients with SARS-CoV-2 in the Kingdom of Bahrain. World J Virol 2021; 10(4):168-81. doi: 10.5501/wjv.v10.i4.168 [Crossref] [ Google Scholar]
- Moreno-García E, Puerta-Alcalde P, Letona L, Meira F, Dueñas G, Chumbita M. Bacterial co-infection at hospital admission in patients with COVID-19. Int J Infect Dis 2022; 118:197-202. doi: 10.1016/j.ijid.2022.03.003 [Crossref] [ Google Scholar]
- Lu Z, Tadi DA, Fu J, Azizian K, Kouhsari E. Global status of azithromycin and erythromycin resistance rates in Neisseria gonorrhoeae: a systematic review and meta-analysis. Yale J Biol Med 2022; 95(4):465-78. [ Google Scholar]
- Gajic I, Kabic J, Kekic D, Jovicevic M, Milenkovic M, Mitic Culafic D. Antimicrobial susceptibility testing: a comprehensive review of currently used methods. Antibiotics (Basel) 2022; 11(4):427. doi: 10.3390/antibiotics11040427 [Crossref] [ Google Scholar]
- Rostami S, Moeineddini L, Ghandehari F, Rahim Khorasani M, Shoaei P, Ebrahimi N. Macrolide-resistance, capsular genotyping and associated factors of group B Streptococci colonized pregnant women in Isfahan, Iran. Iran J Microbiol 2021; 13(2):183-9. doi: 10.18502/ijm.v13i2.5979 [Crossref] [ Google Scholar]
- Akrami S, Abbasi Montazeri E, Saki M, Neisi N, Khedri R, Allah Dini S. Bacterial profiles and their antibiotic resistance background in superinfections caused by multidrug-resistant bacteria among COVID-19 ICU patients from southwest Iran. J Med Virol 2023; 95(1):e28403. doi: 10.1002/jmv.28403 [Crossref] [ Google Scholar]
- Fallah F, Rafiei Tabatabaei S, Yousefi M, Hashemi A, Nazari-Alam A, Saadat A. Association of erythromycin resistance with the mefA and ermB genes among clinical isolates of Streptococcus pneumoniae in Tehran, Iran. Mediterr J Infect Microb Antimicrob 2021; 10(1):19. doi: 10.4274/mjima.galenos.2021.2020.19 [Crossref] [ Google Scholar]
- Roohbakhsh Ghiasi M, Noorbakhsh F, Elikaei A. Evaluation of erythromycin resistant gene in Enterobacteriaceae (Enterobacter, Klebsiella and Proteus) isolated from urine. Iran J Biol Sci 2015; 10(3):11-8. [ Google Scholar]
- Choi J, Rieke EL, Moorman TB, Soupir ML, Allen HK, Smith SD. Practical implications of erythromycin resistance gene diversity on surveillance and monitoring of resistance. FEMS Microbiol Ecol 2018; 94(4):fiy006. doi: 10.1093/femsec/fiy006 [Crossref] [ Google Scholar]