Avicenna Journal of Clinical Microbiology and Infection. 12(1):29-33.
doi: 10.34172/ajcmi.3600
Original Article
Blood Urea Nitrogen and Creatinine Clinical Prognosis in Patients with Severe Coronavirus Disease 19
Hassan Mahmoudi Conceptualization, Data curation, Formal analysis, Funding acquisition, Investigation, Methodology, Project administration, Resources, Software, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing, 1, 2, * 
Mohammad Yousef Alikhani Data curation, Visualization, Writing – original draft, 2
Narges Mofrad Taheri Investigation, Visualization, 3
Alireza Behzadi Investigation, Visualization, 4
Author information:
1Department of Microbiology, Nahavand School of Allied Medical Sciences, Hamadan University of Medical Sciences, Hamadan, Iran
2Infectious Disease Research Center, Avicenna Institute of Clinical Sciences, Avicenna Health Research Institute, Hamadan University of Medical Sciences, Hamadan, Iran
3Department of Internal Medicine, Ayatollah Alimoradiyan Hospital, Nahavand, Hamadan, Iran
4Department of Forensic Medicine and Clinical Toxicity, Ayatollah Alimoradiyan Hospital, Nahavand, Hamadan, Iran
Abstract
Background: COVID-19 is a new respiratory tract infection disease with an evolving understanding of its epidemiology and clinical appearances. Kidney defects seem to be common in patients with COVID-19. In addition, urea and creatinine (Cr) levels often occur at the beginning or during the infection. This evidence shows that COVID-19 also attacks the kidneys. The aim of this study was to evaluate changes in biochemical parameters associated with kidney function, including urea and Cr, in patients with COVID-19.
Methods: A retrospective analysis of the plasma Cr and urea levels of 100 COVID-19 patients with normal plasma Cr and urea was conducted at the first clinical presentation of COVID-19.
Results: Blood urea nitrogen and Cr levels increased in 35 (35%) out of 100 patients with COVID-19 2–4 days after the onset of viral infection. The mean serum urea level and the mean Cr concentration were 34.75±0.10, 37.64±0.32, 39.81±0.10, and 42.56±0.35 mg/dL, as well as 1.50±0.026, 1.51±0.016, 1.99±0.012, and 2.58±0.020 mg/dL, respectively, in the first clinical presentation and 2, 3, and 4 days after the onset of viral infection.
Conclusion: The analysis of Cr and urea levels in patients at the onset of the disease and after 2–4 days revealed that impaired kidney function occurs in COVID-19 patients, and it is one of the leading causes of death in these patients.
Keywords: Coronavirus disease, Respiratory tract infections, Kidney, Creatinine, Urea
Copyright and License Information
© 2025 The Author(s); Published by Hamadan University of Medical Sciences.
This is an open-access article distributed under the terms of the Creative Commons Attribution License (
https://creativecommons.org/licenses/by/4.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Please cite this article as follows: Mahmoudi H, Alikhani MY, Mofrad Taheri N, Behzadi A. Blood urea nitrogen and creatinine clinical prognosis in patients with severe coronavirus disease 19. Avicenna J Clin Microbiol Infect. 2025;12(1):29-33. doi:10.34172/ajcmi.3600
Introduction
On December 31, 2019, a cluster of cases of pneumonia of unknown origin was reported in the city of Wuhan, in Hubei province, China. After a short time, Chinese health authorities confirmed that this cluster was associated with a novel coronavirus 1 and was named coronavirus disease 2019 (COVID-19) in February 2020 by the World Health Organization (WHO). From the beginning of its outbreak until now, COVID-19 has affected more than 143 303 378patients in 221 countries and has become a major global health concern. Overall, 3 050 795people have so far died from COVID-19 as of April 20, 2021. The highest number of mortalities from COVID-19 has been reported in the United States, Brazil, and Mexico, respectively (1-7). COVID-19 has rapidly spread across China and many other countries; therefore, the WHO declared the COVID-19 outbreak as the sixth public health emergency of international concern. Accordingly, health workers, governments, and the public require a coordinated international response to prevent the spread of the disease (5-7). Among patients with confirmed COVID-19, the researchers encountered a significant number of patients with changes in biochemical parameters associated with kidney function (8). According to a recent study, Shi et al have indicated that SARS-CoV-2 interacts with human angiotensin-converting enzyme-II (ACE2) molecules through its spike protein. In addition to the lungs and the heart, the expression of the ACE2 receptor has also been observed in the kidneys (9-12). This study retrospectively analyzed the clinical laboratory information on kidney function from 100 cases of COVID-19 who were admitted into the Ayatollah Alimoradiyan Hospital in Nahavand, Hamadan province, from February 17, 2020, to April 21, 2020.
Methods
Patients and Data Collection
A retrospective analysis was conducted on the plasma creatinine (Cr) and urea levels in the blood of 100 COVID-19 patients with normal plasma Cr and urea at the first clinical presentation of COVID-19 in Ayatollah Alimoradiyan Hospital in Nahavand, Hamadan Province, from February 17, 2020, to April 11, 2020. The samples were collected and retrospectively analyzed. The initial laboratory investigations included complete blood count, erythrocyte sedimentation rate (ESR), arterial blood gas, lactate dehydrogenase (LDH), creatine phosphokinase, C-reactive protein (CRP), liver, and renal function tests. Serial monitoring of the laboratory profile was performed according to the clinical progress of an individual patient. All the patients were laboratory-confirmed positive for COVID-19 by the use of quantitative real-time polymerase chain reaction on throat swab samples. Finally, clinical laboratory findings for all the COVID-19 patients were reviewed, and all information was obtained with a customized data collection form.
Results
Patient Demographic Data
During the study period, 100 patients with confirmed cases of the novel corona virus were admitted to Ayatollah Alimoradiyan Hospital in Nahavand, Hamadan Province. A total of 35 (35%) patients with a mean age of 51 years (20-82) were subsequently found to have elevated plasma Cr and urea levels during the later clinical course. The majority of patients in this study (88.57%) exhibited fever at the time of presentation. A high temperature, defined as a minimum of 38.5°C, was documented in 87% of the patient population (Table 1).
Table 1.
Clinical Characteristics of COVID-19 Patients
Groups
All Patients
(N=100)
|
Patients Without Changes in Urea and Creatinine Levels
n=65 (%)
|
Patients With Changes in Urea and Creatinine Levels
n=35 (%)
|
P
Value
|
| Age (y) |
|
|
|
| ≥ 55 |
42 (64.61) |
29 (82.85) |
0.001 |
| < 55 |
23 (35.39) |
6 (17.15) |
| Gender |
|
|
|
| Male |
45 (69.23) |
24 (68.57) |
0.398 |
| Female |
20 (30.77) |
11 (31.43) |
| Symptoms |
|
|
|
| Fever |
56 (86.15) |
31 (88.57) |
0.0023 |
| Palpitation |
55 (84.61) |
33 (94.28) |
0.0035 |
| Cough |
40(61.53) |
23 (65.71) |
0.0017 |
| Chills |
37 (59.92) |
26 (4.28) |
0.0051 |
| Malaise |
35 (53.84) |
31 (88.57) |
0.0075 |
| Dyspnea |
34 (52.30) |
20 (57.14) |
0.002 |
| Anorexia |
2 (3.07) |
0 (0) |
0.075 |
| Headache |
4 (6.15) |
1 (2.58) |
0.014 |
| Myalgia |
3 (4.61) |
2 (5.71) |
0.034 |
Laboratory Test Findings
All patients had raised levels of high-sensitivity CRP and ESR (100%). In addition, mean serum LDH (350–450 U/l) was increased, especially in those with high baseline serum Cr and urea levels (Figure 1 and Table 2). On the other hand, urea and Cr levels did not differ between male and female patients. However, old patients who developed impaired kidney function had higher urea and Cr levels (P < 0.001, Figure 2).
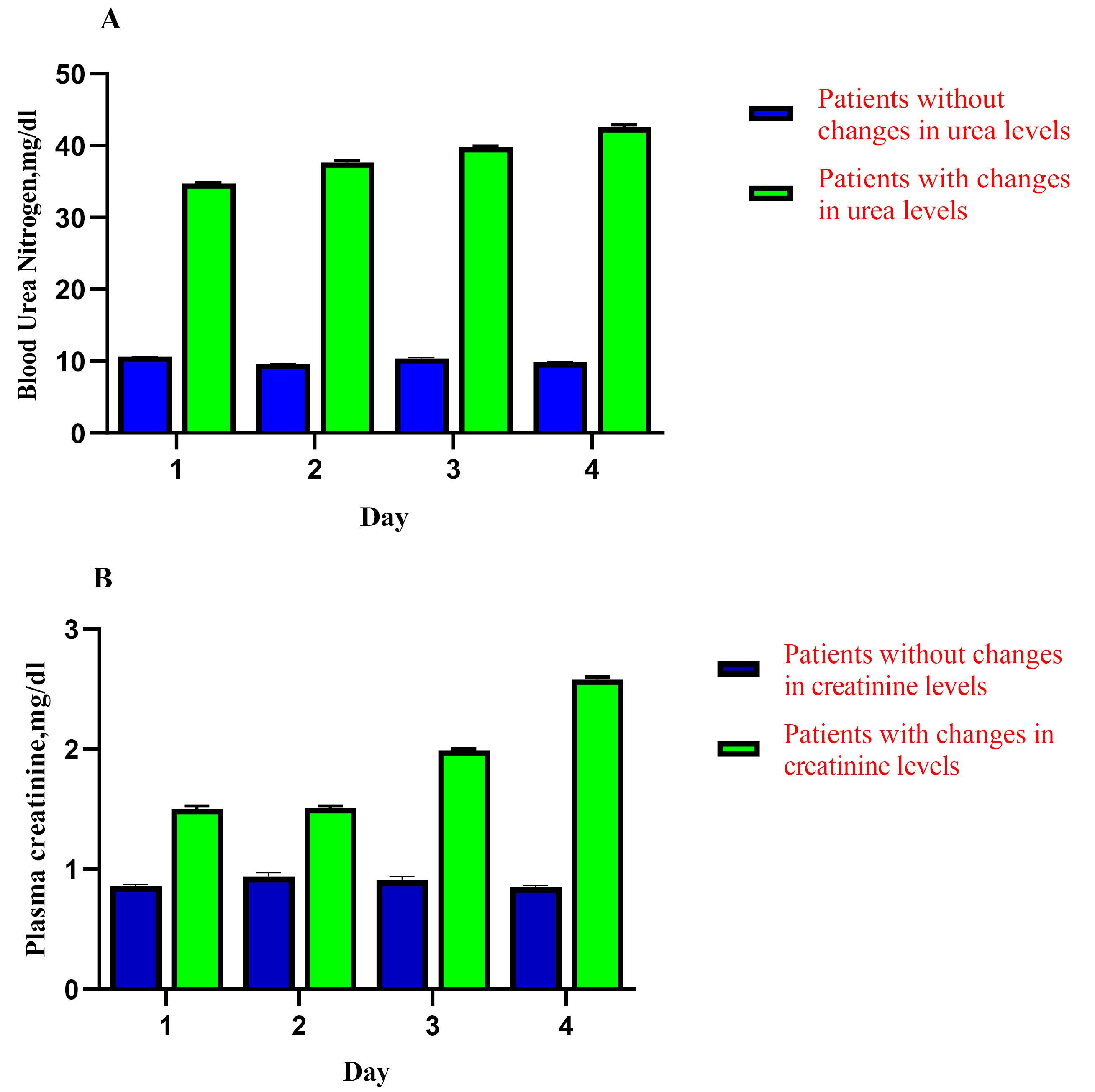
Figure 1.
Differences Between Patients Without and with Changes in Urea and Creatinine Levels
.
Differences Between Patients Without and with Changes in Urea and Creatinine Levels
Table 2.
Changes in BUN and Creatinine Levels in 100 COVID-19-Confirmed Patients
|
COVID-19-Confirmed Patients (N=100)
|
Number
|
BUN, mg/dL (7–20)
|
Creatinine, mg/dL (0.84–1.21)
|
| Patients without changes in urea and creatinine levels |
| First clinical presentation (day 1) |
65 |
10.63 ± 0.02 |
0.86 ± 0.012 |
| Day 2 |
65 |
9.62 ± 0.09 |
0.94 ± 0.032 |
| Day 3 |
65 |
10.40 ± 0.10 |
0.91 ± 0.030 |
| Day 4 |
65 |
9.84 ± 0.09 |
0.85 ± 0.016 |
| Patients with changes in urea and creatinine levels |
| First clinical presentation (day 1) |
35 |
34.75 ± 0.10 |
1.50 ± 0.026 |
| Day 2 |
35 |
37.64 ± 0.32 |
1.51 ± 0.016 |
| Day 3 |
35 |
39.81 ± 0.10 |
1.99 ± 0.012 |
| Day 4 |
35 |
42.56 ± 0.35 |
2.58 ± 0.020 |
|
P value |
|
< 0.0001 |
< 0.0078 |
Note. P-values indicate differences between patients without and with changes in urea and creatinine levels. P< 0.05 was considered statistically significant. BUN: Blood urea nitrogen.
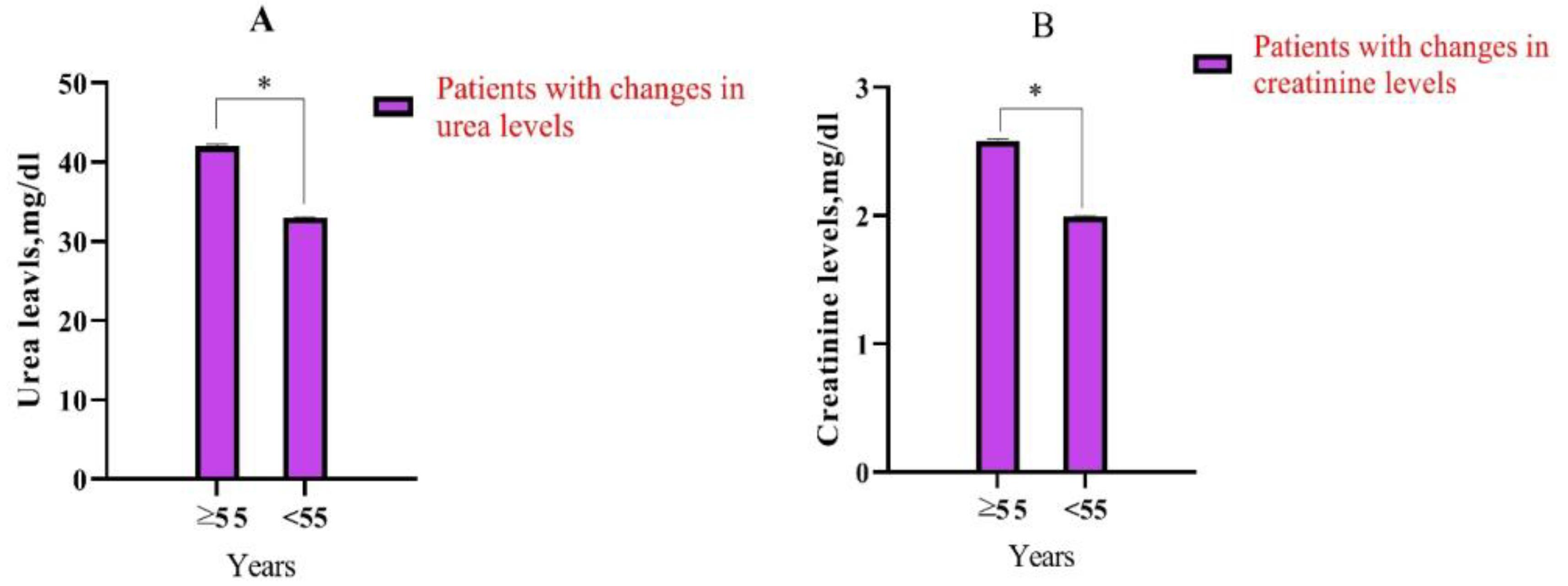
Figure 2.
Differences in the Age (Year) of Patients With Changes in Urea and Creatinine Levels. Note. *P< 0.05 was considered statistically significant.
.
Differences in the Age (Year) of Patients With Changes in Urea and Creatinine Levels. Note. *P< 0.05 was considered statistically significant.
Discussion
COVID-19 is a new respiratory tract infection disease with challenging morbidity and mortality throughout the world. As of February 22, 2020, COVID-19 has killed 96 000 people worldwide. The initial phase of COVID-19 infection is to attach to the host cell receptor and enter the host cells. A varied range of non-respiratory symptoms has consequently been described, suggesting other organ involvements, including the liver, heart, and kidney, during COVID-19 (1-3,9-10).
Kidney damage was described to be a common condition and complication of COVID-19 infection, particularly in patients with severe symptoms (11). The mechanisms of kidney damage caused by SARS-CoV-2 infection are still unclear. The evidence suggests that SARS-CoV-2 may directly affect kidney cells (12). Bourgonje et al reported autopsy data from 12 patients who died of COVID-19, which showed high titers of viral RNA in the kidneys (13). Cheng et al found acute kidney injury (AKI) in 5.1% of COVID-19 patients (14). In our study, we observed that dead patients had a higher proportion of diabetes and high blood urea nitrogen (BUN) and Cr levels compared with surviving patients. Hirsch et al concluded that about 37% of COVID-19 patients advanced AKI, with potential etiology including acute tubular necrosis due to direct viral invasion, cytokine release syndrome, sepsis, and renal hypoperfusion (15).
The new coronavirus can activate the renin-angiotensin-aldosterone system, resulting in decreased renal tubule blood flow and glomerular filtration, thereby leading to reduced BUN excretion, increased absorption of water (H2O) and sodium (Na), and passive BUN reabsorption (16). It is noteworthy that dehydration is common in patients with pneumonia, and BUN reabsorption by the kidneys is increased in the dehydrated state (17). Furthermore, elevated BUN levels reflect inflammatory status, catabolism, nitrogen balance, and renal hypoperfusion resulting from hypovolemia, sepsis, or decreased cardiac output. These pathophysiological changes are closely related to adverse outcomes in COVID-19 patients (18). Pei et al indicated that acute tubular necrosis is the primary reason for AKI in individuals with COVID-19 (19).
Multiple studies have reported that kidney issues arise mostly from AKI, impacting nearly 70% of patients with COVID-19 (20-22). According to Li et al, kidneys were the most affected organs, in addition to the lungs and heart. However, research from the University of Wuhan, China, revealed that among 166 patients hospitalized with COVID-19, 10.35% demonstrated a minor elevation in serum urea or Cr levels, which did not fulfill the AKI criteria (23).
Coronaviruses have a structure of spike protein, which is closely bound to human cell receptor ACE2. Thus, cells with ACE2 expression may act as target cells and are probably sensitive to COVID-19 infection. Recently, Lin et al have found that ACE2 receptor expression in human kidneys represents a potential route of COVID-19 infection (24). Moreover, Fan et al observed that ACE2 receptors are expressed in human kidneys. Yan et al concluded that 63% of COVID-19 patients had a raised level of proteinuria. These results demonstrate that COVID-19-mediated impaired kidney function may be one of the main causes of final death in COVID-19 patients (25). Wang et al reported that 12 (10.8%) patients showed increased BUN or Cr after 2 days. In this study, we found that 35 (35%) of patients with COVID-19 had an increase in Cr and urea levels (Table 1). Over time, the rate of Cr and urea levels increased further (26). Similarly, Li et al (27) presented the data on the clinical characteristics of 1,099 patients with COVID-19. From this study, the renal function revealed that the patients’ number of Cr ≥ 133 μmol/L was 1.6%. These laboratory test findings suggest that impaired kidney function is comparatively common following COVID-19 infection. Recently, some investigators have reported that they have successfully isolated COVID-19 particles from the sample urine of COVID-19 patients, highlighting that kidney-originated viral particles may penetrate the urine via glomerular filtration. The findings of our study and those of other studies confirmed that a human kidney is also a place of COVID-19 infection and replication outside of the lungs (25-27). However, the kidney function of patients with COVID-19 should be regularly monitored, particularly in patients with elevated plasma Cr and urea levels.
Conclusion
The analysis of Cr and urea levels in patients at the onset of the disease and after 2–4 days confirmed that impaired kidney function occurs in COVID-19 patients, and it is considered one of the leading causes of death in this group of patients.
Acknowledgements
The authors would like to appreciate the financial support from the Vice-Chancellor for Research and Technology of Hamadan University of Medical Sciences, Hamadan, Iran.
Competing Interests
The authors declare that they have no competing interests.
Consent for Publication
Personally identifiable data were not collected as part of this study, and no individual-level data are presented within this publication.
Data Availability Statement
The datasets used and analyzed in the current study are available from the corresponding author upon reasonable request.
Ethical Approval
All procedures were approved by Hamadan University of Medical Sciences, Hamadan, Iran (IR.UMSHA.REC.1399.095). The research was performed in accordance with the relevant guidelines and regulations.
Funding
This research was financially supported by the Vice-Chancellor for Research and Technology of Hamadan University of Medical Sciences, Hamadan, Iran.
References
- Lai CC, Shih TP, Ko WC, Tang HJ, Hsueh PR. Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) and coronavirus disease-2019 (COVID-19): the epidemic and the challenges. Int J Antimicrob Agents 2020; 55(3):105924. doi: 10.1016/j.ijantimicag.2020.105924 [Crossref] [ Google Scholar]
- Gorbalenya AE, Baker SC, Baric RS, de Groot RJ, Drosten C, Gulyaeva AA, et al. Severe acute respiratory syndrome-related coronavirus: the species and its viruses–a statement of the Coronavirus Study Group. bioRxiv [Preprint]. February 11, 2020. Available from: https://www.biorxiv.org/content/10.1101/2020.02.07.937862v1.
- Iran COVID - Coronavirus Statistics. https://www.worldometers.info/coronavirus/country/iran/.
- Chen N, Zhou M, Dong X, Qu J, Gong F, Han Y. Epidemiological and clinical characteristics of 99 cases of 2019 novel coronavirus pneumonia in Wuhan, China: a descriptive study. Lancet 2020; 395(10223):507-13. doi: 10.1016/s0140-6736(20)30211-7 [Crossref] [ Google Scholar]
- Huang C, Wang Y, Li X, Ren L, Zhao J, Hu Y. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet 2020; 395(10223):497-506. doi: 10.1016/s0140-6736(20)30183-5 [Crossref] [ Google Scholar]
- Wang C, Horby PW, Hayden FG, Gao GF. A novel coronavirus outbreak of global health concern. Lancet 2020; 395(10223):470-3. doi: 10.1016/s0140-6736(20)30185-9 [Crossref] [ Google Scholar]
- Holshue ML, DeBolt C, Lindquist S, Lofy KH, Wiesman J, Bruce H. First case of 2019 novel coronavirus in the United States. N Engl J Med 2020; 382(10):929-36. doi: 10.1056/NEJMoa2001191 [Crossref] [ Google Scholar]
- Diao B, Wang C, Wang R, Feng Z, Tan Y, Wang H, et al. Human kidney is a target for novel severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infection. medRxiv [Preprint]. April 10, 2020. Available from: https://www.medrxiv.org/content/10.1101/2020.03.04.20031120v4.
- Zhou P, Yang XL, Wang XG, Hu B, Zhang L, Zhang W. A pneumonia outbreak associated with a new coronavirus of probable bat origin. Nature 2020; 579(7798):270-3. doi: 10.1038/s41586-020-2012-7 [Crossref] [ Google Scholar]
- Lin W, Hu L, Zhang Y, Ooi JD, Meng T, Jin P, et al. Single-cell analysis of ACE2 expression in human kidneys and bladders reveals a potential route of 2019-nCoV infection. bioRxiv [Preprint]. February 18, 2020. Available from: https://www.biorxiv.org/content/10.1101/2020.02.08.939892v1.
- Ozturk A, Kara M. Diagnostic and prognostic significance of the lymphocyte/C-reactive protein ratio, neutrophil/lymphocyte ratio, and D-dimer values in patients with COVID-19. Biocell 2022; 46(12):2625-35. doi: 10.32604/biocell.2022.023124 [Crossref] [ Google Scholar]
- Pan XW, Xu D, Zhang H, Zhou W, Wang LH, Cui XG. Identification of a potential mechanism of acute kidney injury during the COVID-19 outbreak: a study based on single-cell transcriptome analysis. Intensive Care Med 2020; 46(6):1114-6. doi: 10.1007/s00134-020-06026-1 [Crossref] [ Google Scholar]
- Bourgonje AR, Abdulle AE, Timens W, Hillebrands JL, Navis GJ, Gordijn SJ. Angiotensin-converting enzyme 2 (ACE2), SARS-CoV-2 and the pathophysiology of coronavirus disease 2019 (COVID-19). J Pathol 2020; 251(3):228-48. doi: 10.1002/path.5471 [Crossref] [ Google Scholar]
- Mahmoudi H. Evaluation of Antibiotics Used in COVID-19 Patients in West of Iran: A Descriptive Study. The Open Microbiology Journal 2023;17. doi: 10.2174/0118742858249570230920110535.
- Hirsch JS, Ng JH, Ross DW, Sharma P, Shah HH, Barnett RL. Acute kidney injury in patients hospitalized with COVID-19. Kidney Int 2020; 98(1):209-18. doi: 10.1016/j.kint.2020.05.006 [Crossref] [ Google Scholar]
- Ok F, Erdogan O, Durmus E, Carkci S, Canik A. Predictive values of blood urea nitrogen/creatinine ratio and other routine blood parameters on disease severity and survival of COVID-19 patients. J Med Virol 2021; 93(2):786-93. doi: 10.1002/jmv.26300 [Crossref] [ Google Scholar]
- Shao M, Li X, Liu F, Tian T, Luo J, Yang Y. Acute kidney injury is associated with severe infection and fatality in patients with COVID-19: a systematic review and meta-analysis of 40 studies and 24,527 patients. Pharmacol Res 2020; 161:105107. doi: 10.1016/j.phrs.2020.105107 [Crossref] [ Google Scholar]
- Mazze RI, Callan CM, Galvez ST, Delgado-Herrera L, Mayer DB. The effects of sevoflurane on serum creatinine and blood urea nitrogen concentrations: a retrospective, twenty-two-center, comparative evaluation of renal function in adult surgical patients. Anesth Analg 2000; 90(3):683-8. doi: 10.1097/00000539-200003000-00032 [Crossref] [ Google Scholar]
- Pei G, Zhang Z, Peng J, Liu L, Zhang C, Yu C. Renal involvement and early prognosis in patients with COVID-19 pneumonia. J Am Soc Nephrol 2020; 31(6):1157-65. doi: 10.1681/asn.2020030276 [Crossref] [ Google Scholar]
- Yang X, Yu Y, Xu J, Shu H, Xia J, Liu H. Clinical course and outcomes of critically ill patients with SARS-CoV-2 pneumonia in Wuhan, China: a single-centered, retrospective, observational study. Lancet Respir Med 2020; 8(5):475-81. doi: 10.1016/s2213-2600(20)30079-5 [Crossref] [ Google Scholar]
- Cheng Y, Luo R, Wang K, Zhang M, Wang Z, Dong L. Kidney disease is associated with in-hospital death of patients with COVID-19. Kidney Int 2020; 97(5):829-38. doi: 10.1016/j.kint.2020.03.005 [Crossref] [ Google Scholar]
- Su H, Yang M, Wan C, Yi LX, Tang F, Zhu HY. Renal histopathological analysis of 26 postmortem findings of patients with COVID-19 in China. Kidney Int 2020; 98(1):219-27. doi: 10.1016/j.kint.2020.04.003 [Crossref] [ Google Scholar]
- Wang L, Li X, Chen H, Yan S, Li D, Li Y. Coronavirus disease 19 infection does not result in acute kidney injury: an analysis of 116 hospitalized patients from Wuhan, China. Am J Nephrol 2020; 51(5):343-8. doi: 10.1159/000507471 [Crossref] [ Google Scholar]
- Fan C, Li K, Ding Y, Lu W, Wang J. ACE2 expression in kidney and testis may cause kidney and testis damage after 2019-nCoV infection. medRxiv [Preprint]. February 13, 2020. Available from: https://www.medrxiv.org/content/10.1101/2020.02.12.20022418v1.
- Cheng Y, Luo R, Wang K, Zhang M, Wang Z, Dong L, et al. Kidney impairment is associated with in-hospital death of COVID-19 patients. medRxiv [Preprint]. February 20, 2020. Available from: https://www.medrxiv.org/content/10.1101/2020.02.18.20023242v1.
- Mahmoudi H. Bacterial co-infections and antibiotic resistance in patients with COVID-19. GMS Hyg Infect Control 2020; 15:Doc35. doi: 10.3205/dgkh000370 [Crossref] [ Google Scholar]
- Li Q, Guan X, Wu P, Wang X, Zhou L, Tong Y. Early transmission dynamics in Wuhan, China, of novel coronavirus-infected pneumonia. N Engl J Med 2020; 382(13):1199-207. doi: 10.1056/NEJMoa2001316 [Crossref] [ Google Scholar]