Avicenna Journal of Clinical Microbiology and Infection. 12(2):86-90.
doi: 10.34172/ajcmi.3590
Original Article
Molecular Identification of Leishmania Species in Kurdistan Province, Western Iran
Mohammad Moghimi Data curation, Formal analysis, Investigation, Software, 1 
Mohammad Matini Validation, Visualization, 1
Amir Hossein Maghsood Methodology, 1
Faeze Foroughi-Parvar Conceptualization, Funding acquisition, Project administration, Resources, Supervision, Writing – original draft, Writing – review & editing, 1, *
Author information:
1Department of Medical Parasitology and Mycology, School of Medicine, Hamadan University of Medical Sciences, Hamadan, Iran
Abstract
Background: Cutaneous leishmaniasis (CL) is regarded as one of the critical public health problems in the tropical and subtropical regions of the world, including Iran. About 20000 annual cases of CL are registered in Iran. Considering the increasing numbers of this parasitic infection in Iran, this study aimed to discover the frequency of CL in western Iran, Kurdistan province, through molecular investigation.
Methods: First, 59 previously confirmed CL-stained Giemsa specimens were examined by two different microscopists, and then polymerase chain reaction (PCR) was performed using two sets of primers (LinR4 and Lin17) to identify the conserved gene region of 18s rRNA for Leishmania major and Leishmania tropica.
Results: Of 59 swab slides, 56 were positive and 3 were negative by the molecular method. Overall, 38 (67.9%, including 35 males and 3 females) and 18 (32.1%, including 18 males) specimens were recognized as L. major and L. tropica, respectively. Those aged 21–30 had the highest incidence of infection (44.64%). In general, 62.5% and 37.5% of people lived in urban and rural areas, respectively. Employees had the highest rate of infection (39.28%). Most cases (12.42 %) had traveled to Mehran (Ilam-Iraq border).
Conclusion: According to the current study, anthroponotic and zoonotic CL is widespread in Kurdistan province. Due to traveling to near borders and endemic areas, there is always a potential risk of spreading this disease. Therefore, disease control planning and continuous monitoring of new cases should always be taken into consideration.
Keywords: Leishmania, Cutaneous leishmaniasis, CL, PCR
Copyright and License Information
© 2025 The Author(s); Published by Hamadan University of Medical Sciences.
This is an open-access article distributed under the terms of the Creative Commons Attribution License (
https://creativecommons.org/licenses/by/4.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Please cite this article as follows: Moghimi M, Matini M, Maghsood AH, Foroughi-Parvar F. Molecular identification of Leishmania species in Kurdistan province, Western Iran. Avicenna J Clin Microbiol Infect. 2025;12(2):86-90. doi:10.34172/ajcmi.3590
Introduction
Cutaneous leishmaniasis (CL) is one of the most serious public health problems in tropical and subtropical countries, including Iran. The global incidence of CL is estimated to be between 600 000 and 1 million annually, and 350 million are at risk of infection worldwide. According to the World Health Organization, in 2023, 6 countries (Afghanistan, Algeria, Brazil, Pakistan, Peru, and the Syrian Arab Republic) reported more than 5000 CL cases, accounting for 83% of global reported CL incidence (1). However, the actual incidence of the infection is much higher than the reported rate, and the number of reports of this vector-borne disease is rising to 20 000 annual cases in Iran (2). The distribution of leishmaniasis is affected by reservoir and vector population and climate changes because Leishmania sp. is an ecosystem-dependent organism (3). CL is endemic to Iran, and 25 out of 31 provinces in Central, West, Southwest, South, Southeast, East, and Northeast are well documented in zoonotic and anthroponotic CL reports (4-7). The diagnosis of CL is essentially based on clinical symptoms and parasitological methods, including direct microscopic examination of lesions and culture. Molecular methods, such as polymerase chain reaction (PCR), are widely used to find small amounts of DNA parasites, even in chronic skin lesions with low parasite density (8). The wide spectrum of clinical manifestations, diversity of Leishmania species, and problematic responses to treatment have resulted in identifying much more sensitive methods of studying Leishmania parasites (9). Considering that Kurdistan province has outlined a high frequency of CL areas, it is critical to determine the frequency of this parasitic disease in this area. Therefore, this study was conducted to investigate the epidemiological aspects of CL in Kurdistan province.
Materials and Methods
Area
Kurdistan province (Figure 1), with an area of 28 023 km2 in western Iran, borders Iraq to the west, West Azerbaijan province to the north, Zanjan province to the northeast, Hamadan to the east, and Kermanshah to the south. It lies between the latitudes 34º and 44º to 36º and 30º north and the longitudes 45º and 31º to 48º and 16º east. As the 16th province of Iran in terms of area, Kurdistan occupies 1% of the total area of Iran. Kurdistan province is a mountainous region with plateaus and wide valleys. The difference between the highest and lowest parts of the province is about 2400 m. Many rivers originate from the mountains of Kurdistan province, connected to the Caspian Sea and Lake Urmia (10).
Sampling
A total of 59 previously confirmed CL-stained Giemsa specimens were randomly collected from different health centers and hospitals in Kurdistan province. Conventional microscopic examinations were separately performed by two microscopists to verify amastigotes at 1000x magnification.
Molecular Identification
The smear on the slides was gently scraped into a 1.5 mL sterile Eppendorf tube, and then Chelex solution (100 µL of a 5% stock solution) was added to it. These tubes were incubated at 56 °C for 10 minutes and then vortexed. This step was repeated once more, and the Chelex suspension was heated in a boiling water bath at 100 °C for 10 minutes. Finally, the tubes were centrifuged at 12 000 rpm for 3 minutes at room temperature. The supernatant was carefully drained to avoid the Chelex combination. The quality of the extracted DNA was evaluated in 260–280 nm spectrometry (Nanodrop 1000; ND 1000 V3.8.1, Thermo Fisher) according to previous research (11,12).
PCR was performed using two sets of primers, LinR4 and Lin17 (Table 1), to identify the conserved gene region of 18s rRNA. The specificity of the primer pairs was checked by the National Center for Biotechnology Information Basic Local Alignment Search Tool. Each PCR cycle included an initial denaturation at 95 °C for 6 minutes, 30 cycles of denaturation at 94 °C for 30 seconds, annealing at 56 °C for 30 seconds, and extension at 72 °C for 40 seconds. PCR products were analyzed using 1.5% agarose gel electrophoresis.
Table 1.
Specific Primer Sequences of LinR4 and Lin17
|
Name of the Primer
|
5'-3' Sequence
|
Amplification Size (bp)
|
| LinR4 |
GGGGTTGGTGTAAAATAGGG |
760 bp (for Leishmania tropica)
650 bp (for Leishmania major) |
| Lin17 |
TTTGAACGGGATTTCTG |
|
The statistical analysis was conducted with SPSS (version 16; IBM Corporation, Armonk, NY, USA). Variables were analyzed by the Chi-square test. All data were presented as means and standard deviations (SD), and the level of statistical significance was set at P < 0.05.
Results
A total of 59 stained slides were collected from health centers of Kurdistan province as positive cases of leishmaniasis. It was found that 93.2% (55 out of 59 slides) were microscopically positive for Leishmania sp. Of 59 slides, 56 were PCR-positive, and the remaining 3 were PCR-negative. Leishmania major was detected in 38 specimens (67.9%, including 35 males and 3 females, P = 0.546), while 18 specimens (32.1%, including 18 males) were recognized as Leishmania tropica. Using LinR4 and Lin17 primers, bands of 760 bp and 650 bp were generated in gel electrophoresis, determining L. tropica and L. major, respectively (Figure 2).
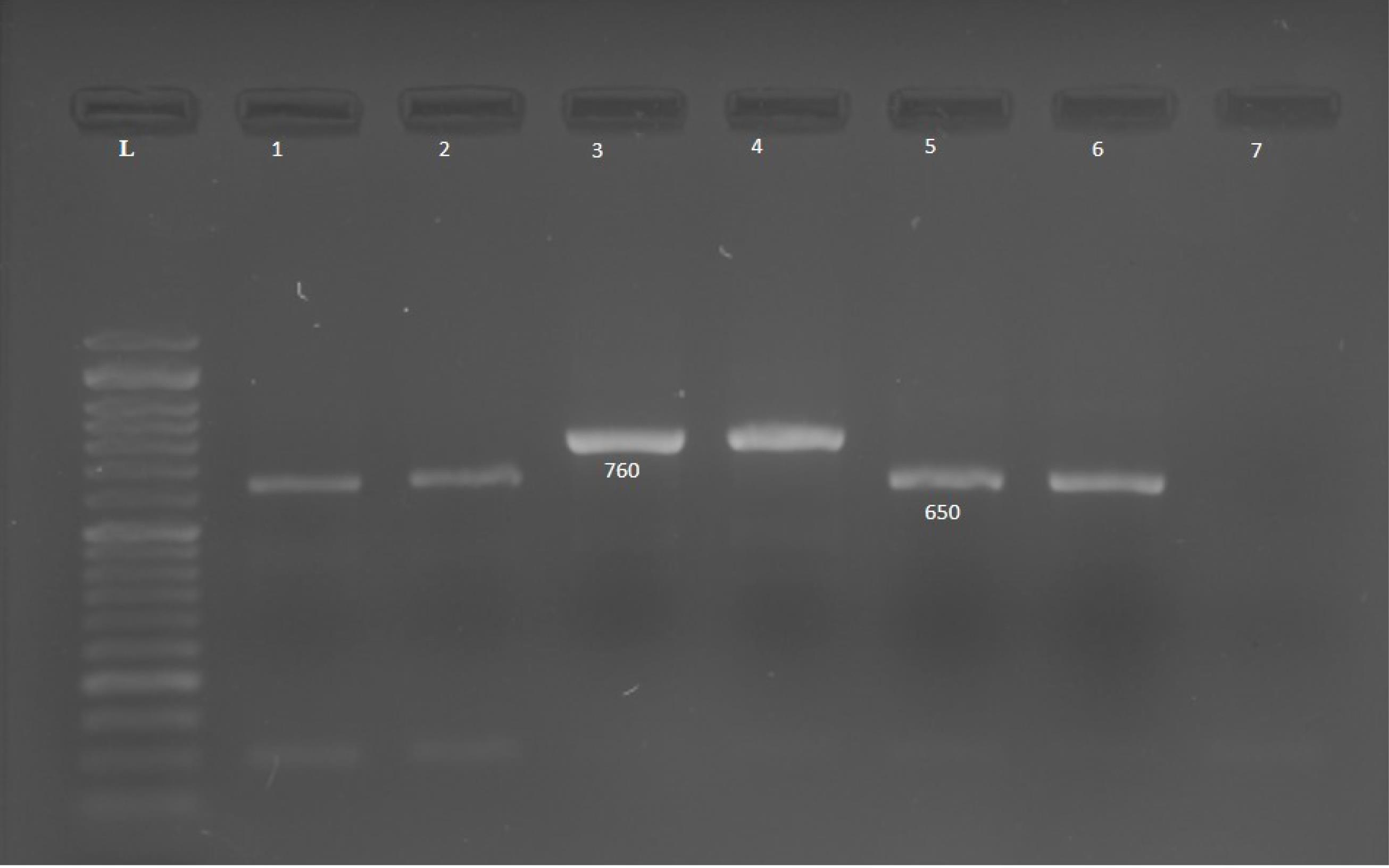
Figure 2.
Electrophoresis of PCR Products Using Leishmania Species-Specific Primers (LinR4 and Lin17) in 1.5% Agarose Gel. Note. PCR: Polymerase chain reaction; L: 100 bp marker, 1: L. major standard (650 bp), 2: Patient sample (L. major), 3: Standard (L. tropica) (760 bp), 4: Patient sample (L. tropica). 5: L. major standard (650 bp), 6: Patient sample (L. major), and 7: Negative control. L. tropica: Leishmania tropica; L. major: Leishmania major
.
Electrophoresis of PCR Products Using Leishmania Species-Specific Primers (LinR4 and Lin17) in 1.5% Agarose Gel. Note. PCR: Polymerase chain reaction; L: 100 bp marker, 1: L. major standard (650 bp), 2: Patient sample (L. major), 3: Standard (L. tropica) (760 bp), 4: Patient sample (L. tropica). 5: L. major standard (650 bp), 6: Patient sample (L. major), and 7: Negative control. L. tropica: Leishmania tropica; L. major: Leishmania major
The anthroponotic form of CL accounted for the majority (73.3%) of the lesions, with L. major and L. tropica detected as 68.3% and 31.7%, respectively (P = 0.783). Hands and arms were the most popular sites (62%) for sandfly bites (P = 0.63). Overall, 62.7% of cases had less than 2 lesions (P = 0.62). The topical injection of glucantime was used for more than 67.86% of the other treatment modalities, including oral treatment or cryotherapy. Most of the examined slides (44.64%) belonged to the age group of 21–30 years (P = 0.22), and 76% and 24% of this age group were infected by L. major and L. tropica, respectively. Of the total subjects, 62.5% lived in urban areas, while 37.5% resided in rural areas (P = 0.592). Moreover, 31.42% (11 out of 35) and 68.58% (24 out of 35) of townspeople were infected by L. tropica and L. major, respectively. Staff members were the most infected group (39.28%, 22 of 56 cases). The lowest infection rate was reported among housewives (3.07%, 2 out of 56 cases, P = 0.458). In terms of movements, the most positive cases of infection (12.42%, 12 of 56, including 10 L. major and 2 L. tropica, P = 0.22) had a history of trips to Mehran, Iran. At the next level, 17.85% (10 out of 56) of people referred to Ilam province (no specific area), Iran, as their travel history. In addition, most positive cases of L. tropica (n = 5) had traveled to Kurdistan province (Iran) in the past.
Using Fisher’s exact and chi-square tests, no significant relationship was observed between the frequency and variables.
Discussion
It is highly recommended that Leishmania species be identified to understand the distribution of infection, the reservoir host, and the establishment of preventive, control, or therapeutic measures. DNA parasite identification has been regarded as an effective method in recent years due to sensitivity, specificity, and species diagnosis (13-15).
The PCR method via two highly conserved primers was used for the characterization of Leishmania species on Giemsa-stained slides. According to the results, 55 out of 59 samples were recognized as positive on microscopic examination. The molecular method identified 56 positive cases out of 59. Out of 4 confirmed negative cases by the microscopic method, 3 were re-confirmed negative, while 1 was determined positive by molecular examination. It should be noted that although the microscopic examination is the gold standard method for the diagnosis of CL, there is always a possibility of examiner error due to the small number of parasites on the slide. Furthermore, based on the guidelines, three slides were allocated to each patient, and the exclusive slide (detected for Leishmania) might have had low-scored amastigotes, while the slide diagnosed at the relevant health center would be microscopically positive.
The cold and mountainous climate of Kurdistan province has created a non-endemic region in terms of CL life cycle. Most of the infected people had traveled to other regions in the past; for example, the highest incidence of traveling was related to the Mehran region on the border with Iraq. In studies conducted in Iraq by Hassan and Hussein, it was found that the number of CL cases in this region is increasing annually (16,17). There are no reliable statistics on the annual incidence of CL in Kurdistan province, but the annual incidence in 2013 in adjacent provinces, such as Ilam, Kermanshah, Hamadan, and West Azerbaijan, was reported to be 102.64, 3.47, 2.98, and 0.77, respectively, per 100 000 per cases (18). Perhaps, in recent years, molecular-sensitive methods in detecting DNA parasites have shown much more positive results compared to microscopic techniques (19).
In the present study, 56 out of 59 cases were molecularly identified as positive, 18 of them as L. tropica and 38 as L. major. L. major has been reported in both genders, while L. tropica has only been detected in males. No significant gender differences were reported in this study, which is in line with the results of studies performed by Mohajery et al in Neishabour (20), Fata et al in Fariman, Mashhad (21), Mohajery et al in Mashhad (22), and Maghsoud et al in Pakdasht (23). However, studies by Aflatoonian et al (24) and Ebadi and Hejazi (25) found that there is a significant association between gender and CL. A simple reason could be the fact that women cover their bodies a lot more than men. Moreover, males come into contact with sandflies since they spend more time outdoors compared to females.
Given the current results indicating that approximately 68.86% of cases were confirmed as L. major, most lesions were expected to be moist. The reason may be a lack of knowledge of the nature of the wound by some medical professionals who recorded a wet wound as a dry wound. The anatomical localization of the CL lesion was observed in the hands and arms in most patients (32.14%), while the least number of wounds was detected in the trunk. These results confirmed that sandflies are unable to bite clothing and are often attracted to open areas of the body to take a blood meal (26). They are also less common in the facial area because the person consciously prevents mosquito bites. In this respect, the present results confirm to those of Rahmanian et al (27) and Abbasi et al (28). The majority of cases had only one affected organ, and 62.7% of cases had multiple (two) lesions, suggesting that sandflies may bite the host at multiple sites in search of blood (28,29).
All patients were successfully treated, and the topical injection of glucantime healed 67.8% of CL cases. Several methods, such as cryotherapy or heat therapy, have been used to treat CL. Due to the difficulty of these procedures and the non-endemic nature of Kurdistan province (Iran), topical injection methods are the most common techniques utilized to treat the disease. In agreement with the present study, Spotin et al confirmed that most patients improved by the local administration of glucantime since the effect of the drug on the parasite is fast and effective with this method (30).
Most positive cases belonged to the 21–30 age group, consistent with other findings from studies across the country (23,27,31). The activity of this age group is increased outdoors when sandflies remain active from sunset until late at night, and they are exposed to mosquito bites.
There were 35 urban and 21 rural residents who had a travel history to various destinations. One of the potent factors in the prevalence and incidence of CL is traveling to endemic areas of CL. Previous studies demonstrated that some areas, such as Isfahan (32), the northern cities of Iran, the Turkmen Sahara (33), Mashhad (20), and Neishaboor (22), are considered endemic regions for CL; thus, moving between endemic areas may increase the risk of infection. In the present study, most patients had traveled to Mehran (Ilam province, Iran). Others had various destinations to other places of Ilam province (Iran), Ahvaz (Iran), Mashhad (Iran), and Karbala (Iraq). In general, the transmission of infection occurred in close quarters at the border points of the country.
In this study, most patients were staff members. However, in the study performed by Hatam et al (34), patients were drivers. Further investigation revealed that employees of governmental and non-governmental agencies have prolonged exposure to Phlebotomus sp. bites because of various missions inside or outside the province. No significant relationship was observed between the variables.
Conclusion
In summary, most samples were identified as L. major. While the low incidence of CL in Kurdistan province is not deemed a significant health concern, the potential for transmission to endemic regions poses a risk for the establishment of a transmission cycle and the spread of infection. Furthermore, microscopic techniques are suitable for quick detection or field screening studies, whereas molecular methods are preferred for identifying Leishmania species. Although molecular techniques are more expensive than microscopic methods, they require less time compared to the culture media approach for species identification (35). Determining whether leishmaniasis is transmitted from humans to humans (anthroponotic) or from animals to humans (zoonotic) is crucial for developing effective treatment strategies, prevention techniques, vector management, and broader regional health policies. Consequently, it is imperative to prioritize the planning and implementation of necessary preventive health initiatives in the Kurdistan province, Iran.
One of the limitations of this project was the reduction in the number of samples due to the project’s time constraint. On the other hand, regarding the use of specific primers for conventional PCR, the results have been obtained in less time for accurate species identification, along with cost-efficiency and material savings.
Acknowledgements
We would like to appreciate the Vice-Chancellor for Research and Technology, Hamadan University of Medical Sciences, for financial support (Project No. 9908065472). In addition, special thanks go to Dr. Seyed Mousa Motevalli Haghi and Mehran Bakhtiari for their technical support.
Competing Interests
The authors declare that they have no conflict of interests.
Ethical Approval
The authors declare that they have obtained appropriate institutional review board approval or have followed the principles outlined in the Declaration of Helsinki for all human or animal experimental investigations (Ethical code IR.UMSHA.REC.1399.551).
Funding
The study was financially supported by the Office of theVice-Chancellor for Research and Technology, Hamadan University of Medical Sciences (Project No. 9908065472).
References
- World Health Organization (WHO). Leishmaniasis. Available from: https://www.who.int/data/gho/data/themes/topics/gho-ntd-leishmaniasis.
- Shirzadi MR, Gouya MM. National Guidelines for Cutaneous Leishmaniasis Surveillance in Iran. Ministry of Health Zoonoses Control Dep Tehran, Iran; 2012.
- World Health Organization (WHO). Leishmaniasis. 2021. Available from: https://www.who.int/news-room/fact-sheets/detail/leishmaniasis.
- Ghatee MA, Taylor WR, Karamian M. The geographical distribution of cutaneous leishmaniasis causative agents in Iran and its neighboring countries, a review. Front Public Health 2020; 8:11. doi: 10.3389/fpubh.2020.00011 [Crossref] [ Google Scholar]
- Izadi S, Mirhendi H, Jalalizand N, Khodadadi H, Mohebali M, Nekoeian S. Molecular epidemiological survey of cutaneous leishmaniasis in two highly endemic metropolises of Iran, application of FTA cards for DNA extraction from Giemsa-stained slides. Jundishapur J Microbiol 2016; 9(2):e32885. doi: 10.5812/jjm.32885 [Crossref] [ Google Scholar]
- Kolivand M, Fallah M, Salehzadeh A, Davari B, Poormohammadi A, Pazoki Ghohe H. An epidemiological study of cutaneous leishmaniasis using active case finding among elementary school students in Pakdasht, southeast of Tehran, Iran 2013-2014. J Res Health Sci 2015; 15(2):104-8. [ Google Scholar]
- Karamian M, Kuhls K, Hemmati M, Ghatee MA. Phylogenetic structure of Leishmania tropica in the new endemic focus Birjand in east Iran in comparison to other Iranian endemic regions. Acta Trop 2016; 158:68-76. doi: 10.1016/j.actatropica.2016.02.010 [Crossref] [ Google Scholar]
- Montalvo AM, Alba A, Fraga J, Marzoa A, Torres C, Muskus C. Improving the sensitivity of an Hsp20-based PCR for genus detection of Leishmania parasites in cutaneous clinical samples: a proof of concept. Parasitol Res 2020; 119(1):345-9. doi: 10.1007/s00436-019-06520-6 [Crossref] [ Google Scholar]
- Pourmohammadi B, Motazedian M, Hatam G, Kalantari M, Habibi P, Sarkari B. Comparison of three methods for diagnosis of cutaneous leishmaniasis. Iran J Parasitol 2010; 5(4):1-8. [ Google Scholar]
- Sadeghi M, Malekian M, Khodakarami L. Forest losses and gains in Kurdistan province, western Iran: where do we stand?. Egypt J Remote Sens Space Sci 2017; 20(1):51-9. doi: 10.1016/j.ejrs.2016.07.001 [Crossref] [ Google Scholar]
- Singh UA, Kumari M, Iyengar S. Method for improving the quality of genomic DNA obtained from minute quantities of tissue and blood samples using Chelex 100 resin. Biol Proced Online 2018; 20:12. doi: 10.1186/s12575-018-0077-6 [Crossref] [ Google Scholar]
- Kheirandish F, Chegeni Sharafi A, Kazemi B, Mohebali M, Sarlak A, Tarahi MJ. Identification of leishmania species using PCR assay on Giemsa-stained slides prepared from cutaneous leishmaniasis patients. Iran J Parasitol 2013; 8(3):382-8. [ Google Scholar]
- Murray HW, Berman JD, Davies CR, Saravia NG. Advances in leishmaniasis. Lancet 2005; 366(9496):1561-77. doi: 10.1016/s0140-6736(05)67629-5 [Crossref] [ Google Scholar]
- Chang KP, Fong D, Bray RS. Biology of Leishmania and leishmaniasis. In: Chang KP, Bray ES, eds. Leishmaniasias. Netherlands, Amesterdam: Elsevier; 1985. p. 1-30.
- Mbow ML, Bleyenberg JA, Hall LR, Titus RG. Phlebotomus papatasi sand fly salivary gland lysate down-regulates a Th1, but up-regulates a Th2, response in mice infected with Leishmania major. J Immunol 1998; 161(10):5571-7. [ Google Scholar]
- Hassan ZI. Molecular characterization of cutaneous leishmaniasis isolated from human in Erbil province-Kurdistan region/Iraq. Zanco J Pure Appl Sci 2018; 30(2):76-85. [ Google Scholar]
- Hussein NR, Balatay AA, Saleem ZS, Hassan SM, Assafi MS, Sheikhan RS. A clinical study of cutaneous leishmaniasis in a new focus in the Kurdistan region, Iraq. PLoS One 2019; 14(5):e0217683. doi: 10.1371/journal.pone.0217683 [Crossref] [ Google Scholar]
- Norouzinezhad F, Ghaffari F, Norouzinejad A, Kaveh F, Gouya MM. Cutaneous leishmaniasis in Iran: results from an epidemiological study in urban and rural provinces. Asian Pac J Trop Biomed 2016; 6(7):614-9. doi: 10.1016/j.apjtb.2016.05.005 [Crossref] [ Google Scholar]
- Arnheim N, White T, Rainey WE. Application of PCR: organismal and population biology. Bioscience 1990; 40(3):174-82. doi: 10.2307/1311362 [Crossref] [ Google Scholar]
- Mohajery M, Hajaran H, Shamsian A, Tavakol Afshari J, Sasabadi F. Detecting Leishmaniasis agents in Nieshabour using RAPD-PCR technique. Med J Mashhad Univ Med Sci 2008;51:74-86. [Persian].
- Fata A, Moghaddas E, Rezee A, Abdali A, Jarahi L, Shamsian A. Epidemiological study of cutaneous leishmaniasis and identification of etiological species. J Mazandaran Univ Med Sci 2018;27(158):123-31. [Persian].
- Mohajery M, Boloursaz M, Shamsian A. Evaluation of cutaneous leishmaniasis among students in Mashhad. Med J Mashhad Univ Med Sci 2001;44:54-60. [Persian].
- Maghsoud A, Pourmohamadi A, Hoseinizijvad M, Tavakoli G, Kolivand M. Survey prevalence of cutaneous leishmaniasis in Pakdasht county in 2012. Pajouhan Sci J 2014;12(2):37-46. [Persian].
- Aflatoonian MR, Sharifi I, Aflatoonian B, Bamorovat M, Heshmatkhah A, Babaei Z. Associated-risk determinants for anthroponotic cutaneous leishmaniasis treated with meglumine antimoniate: a cohort study in Iran. PLoS Negl Trop Dis 2019; 13(6):e0007423. doi: 10.1371/journal.pntd.0007423 [Crossref] [ Google Scholar]
- Ebadi M, Hejazi H. The epidemiological study of cutaneous leishmaniaisis situation in the students of primary school in Isfahan Borkhar region. J Kerman Univ Med Sci 2003;10(4):92-8. [Persian].
- Sarwar M. Typical flies: natural history, lifestyle and diversity of Diptera. In: Sarwar M, ed. Life Cycle and Development of Diptera. IntechOpen; 2020. doi: 10.5772/intechopen.91391.
- Rahmanian V, Rahmanian K, Sarikhani Y, Sotoodeh Jahromi A, Madani A. Epidemiology of cutaneous leishmaniasis, west south of Iran, 2006-2014. J Res Med Dent Sci 2018; 6(2):378-83. doi: 10.5455/jrmds.20186258 [Crossref] [ Google Scholar]
- Abbasi A, Ghanbary MR, Kazem Nezhad N. The epidemiology of cutaneous leishmaniasis in Gorgan (1998-2001). Ann Mil Health Sci Res 2004;2(1):275-8. [Persian].
- Karami M, Doudi M, Setorki M. Assessing epidemiology of cutaneous leishmaniasis in Isfahan, Iran. J Vector Borne Dis 2013; 50(1):30-7. [ Google Scholar]
- Spotin A, Rouhani S, Ghaemmaghami P, Haghighi A, Zolfaghari MR, Amirkhani A. Different morphologies of Leishmania major amastigotes with no molecular diversity in a neglected endemic area of zoonotic cutaneous leishmaniasis in Iran. Iran Biomed J 2015; 19(3):149-59. doi: 10.7508/ibj.2015.03.004 [Crossref] [ Google Scholar]
- Aflatoonian MR, Sharifi I. The epidemiology of cutaneous leishmaniasis in the city and suburb of Bam in 2010: active case-finding, treatment and health education of the school children. Iran J Epidemiol 2011; 7(3):52-7. [ Google Scholar]
- Momeni AZ, Aminjavaheri M. Clinical picture of cutaneous leishmaniasis in Isfahan, Iran. Int J Dermatol 1994; 33(4):260-5. doi: 10.1111/j.1365-4362.1994.tb01039.x [Crossref] [ Google Scholar]
- Mozafari O, Sofizadeh A, Shoraka HR. Distribution of Leishmania infection in humans, animal reservoir hosts and sandflies in Golestan province, northeastern Iran: a systematic review and meta-analysis. Iran J Public Health 2020; 49(12):2308-19. doi: 10.18502/ijph.v49i12.4813 [Crossref] [ Google Scholar]
- Hatam GR, Rezanezhad H, Motazedian MH, Sarkari B. In vitro infectivity of Leishmania major isolated from patients with different clinical forms of cutaneous leishmaniasis and its association with parasite zymodems. Iran J Parasitol 2009; 4(3):52-60. [ Google Scholar]
- Kazemi-Rad E, Mohebali M, Hajjaran H, Rezaei S, Mamishi S. Diagnosis and characterization of Leishmania species in Giemsa-stained slides by PCR-RFLP. Iran J Public Health 2008; 37(1):54-60. [ Google Scholar]