Avicenna Journal of Clinical Microbiology and Infection. 12(1):47-55.
doi: 10.34172/ajcmi.3580
Review Article
Monkeypox: Difficulties and Prospects for Worldwide Disease Management
Dorna Rafighi Writing – original draft, 1 
Sina Samenezhad Formal analysis, 2
Ali Khodadadeh Jigheh Investigation, Project administration, 3, *
Author information:
1Department of Microbiology, Sciences and Research Branch, Islamic Azad University, Tehran, Iran
2Urology Department, School of Medicine, Shahid Beheshti University of Medical Sciences, Tehran, Iran
3Department of Microbiology, Central Tehran Branch, Islamic Azad University, Tehran, Iran
Abstract
Monkeypox (MPX) has become a global public health problem. This zoonotic viral disease, characterized by rash, lymphadenopathy, and fever, used to be restricted to Central and West Africa. However, recent outbreaks have increased its global reach. This study examined the problems and opportunities for MPX control. Articles published from 2013 to 2023 were included in this investigation while excluding the ones that were unavailable in the general library or were only available in conference abstract form. MPX is transmitted through close contact with infected animals. Medically proven, it can be tested with polymerase chain reaction (PCR). Nonetheless, there is no specific treatment for this type of disease. Only supportive measures can be taken in this regard, and smallpox vaccination offers some protection against MPX. Accordingly, international financial support should be allocated to studies on this disease in order to develop safer vaccines, take more holistic health approaches to prevent human-to-human transmission, and put suitable surveillance systems in place.
Keywords: Monkeypox, Epidemic control, Public health, Health challenges, Diagnosis
Copyright and License Information
© 2025 The Author(s); Published by Hamadan University of Medical Sciences.
This is an open-access article distributed under the terms of the Creative Commons Attribution License (
https://creativecommons.org/licenses/by/4.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Please cite this article as follows: Rafighi D, Samenezhad S, Khodadadeh Jigheh A. Monkeypox: difficulties and prospects for worldwide disease management. Avicenna J Clin Microbiol Infect. 2025;12(1):47-55. doi:10.34172/ajcmi.3580
Introduction
The monkeypox virus (MPXV) is the cause of monkeypox (MPX). This infectious disease is zoonotic and transmissible between humans and animals and has recently emerged as a major global public health concern. Similar to smallpox, symptoms typically include fever, headache, skin rash, lymphadenopathy, and blisters (1,2). MPXV is a member of the genus Orthopoxvirus and the family Poxviridae. Its genome is double-stranded DNA (3,4). Rats, squirrels, and monkeys are among the animals that can infect people with this virus. Close contact with the bodily fluids of the infected animal, such as saliva, skin sores, or mucous membranes, may cause MPX. Serious side effects, such as pneumonia and sepsis, can arise from severe infections (1).
The pathogen, found in West and Central Africa, comprises two different genetic clades that cause disease. Based on initial evidence, the Central African (Congo Basin) clade results in more severe disease than the Western clade. Currently, the Western clade is more frequently observed in those who have come into contact with the virus (2,3). The first recorded human case of MPX occurred in 1970, although the initial cases of the virus were reported in Africa in 1958. Due to recent reports of MPX cases worldwide, the World Health Organization (WHO) declared MPX a public health emergency of international concern in 2022. According to a report from the WHO in January 2023, 103 countries reported their first cases of MPX. The United States, Brazil, Peru, Nigeria, Mexico, Spain, Chile, Ecuador, Argentina, and Belgium were the top eight countries with reported deaths linked to MPX (4), the details of which are displayed in Figure 1.
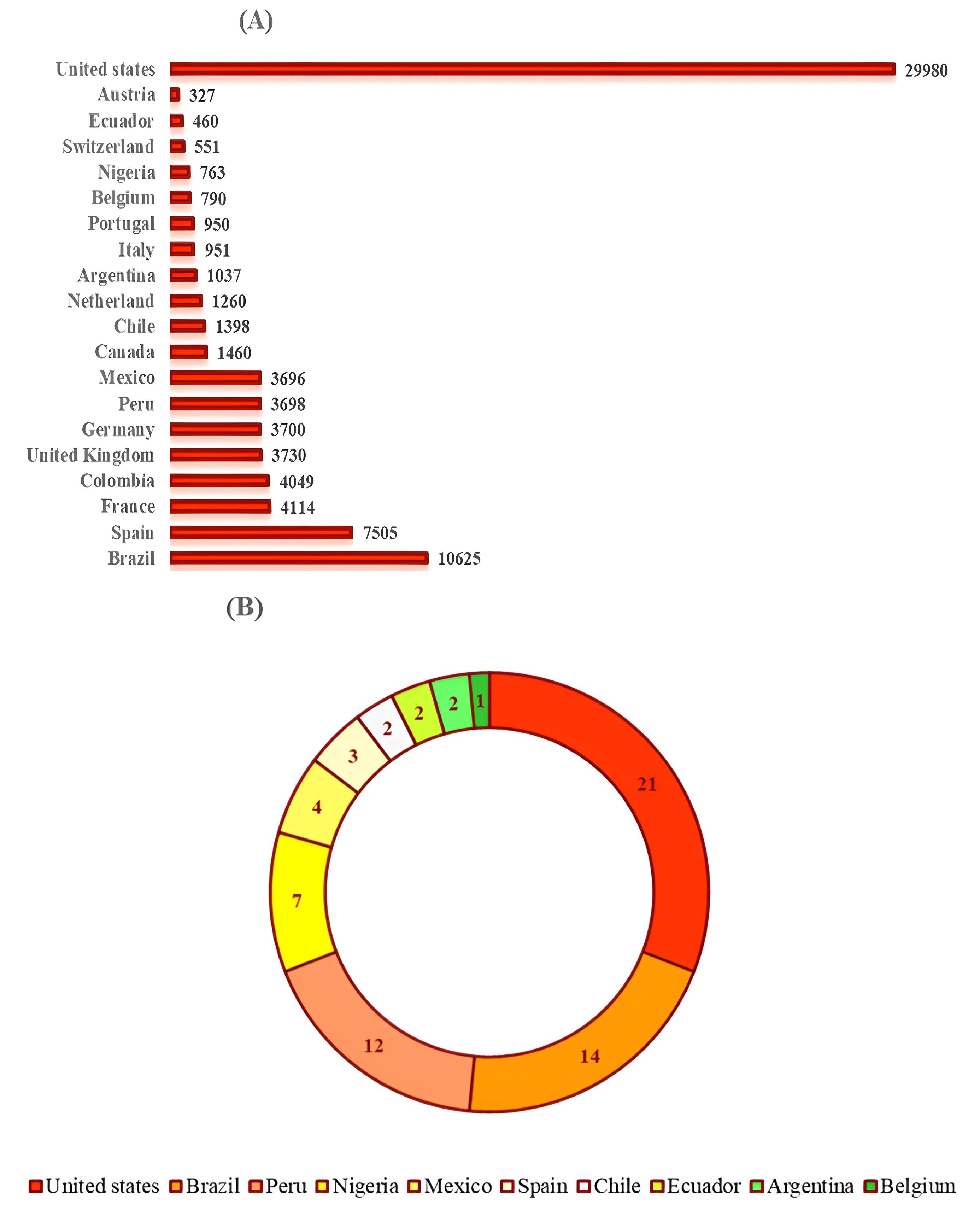
Figure 1.
The Global Breakdown of Monkeypox Cases (A) and Deaths (B) per Nation as of January 2023. Note. The number of deaths is represented by the size of each segment in the pie chart
.
The Global Breakdown of Monkeypox Cases (A) and Deaths (B) per Nation as of January 2023. Note. The number of deaths is represented by the size of each segment in the pie chart
MPX has become a significant international health issue in the last few years. Now, more than ever, extensive and comprehensive research is needed on this disease due to the rising number of patients across numerous continents and the WHO’s announcement of a state of emergency. This review paper aims to provide a thorough and up-to-date examination of MPX and associated challenges and highlight some potential new directions for managing this condition. This article will also discuss the epidemiology, pathophysiology, diagnosis, therapy, and prophylaxis of MPX, as well as an assessment of the current situation and future possibilities for controlling the disease.
Pertinent articles on MPX published between January 2013 and December 2023 were sought in the PubMed, Scopus, and Google Scholar databases. To facilitate this process, several key terms were used, including MPX, epidemiology, morphology, pathophysiology, treatment, control, and complications of the disease. Overall, 83 preliminary articles were found as a result of this search. For a more detailed analysis, articles were selected whose full texts were provided free of charge. Therefore, out of the 83 original articles, 53 full-text, open-access articles were chosen for further examination. Articles published solely as conference abstracts or those behind a paywall for reading the full text were not included in this study. This selection criterion was applied to focus on literature that was easily accessible along with its complete content to facilitate more in-depth analysis.
Epidemiology of Monkeypox Virus
In 1970, MPX was originally discovered in the Congo. About 59 cases of this illness were documented in the western and central parts of Africa in the 1970s. The death rate of MPX has increased to 17%, making it especially harmful for children under the age of ten. Three major MPX epidemics occurred in the Democratic Republic of the Congo between 2000 and 2015; around 760 cases were confirmed by laboratory testing during this time (5). After an almost 40-year hiatus, MPX has returned to Nigeria since 2017, with thousands of cases mostly in the southern areas (6).
Historical boundaries of MPX in central and western Africa have recently been breached by a global outbreak. Although young children were historically more susceptible in Africa, the new epidemics have affected a wider age group, including adults. Notably, men have been disproportionately impacted in non-African regions (7,8). While MPX outbreaks primarily occur in Nigerian metropolitan centers, the disease is predominantly prevalent in rural villages bordering the equatorial rainforest in the Democratic Republic of the Congo. This is likely due to increased human-animal interaction (6,9). Research suggests that the diversity of animal hosts that can be affected by MPX may explain why outbreak patterns vary across different geographical areas. This diversity increases the risk of indirect zoonotic transmission by aiding the virus in adapting to different habitats (9).
According to a WHO report from 2022, 1284 cases of probable MPX were reported in the Congo between January and May (5). A few isolated instances have also been documented in other nations, including the United States, the United Kingdom, and Singapore, in addition to the increasing number of cases in the endemic African nations. Numerous cases that have been documented in these nations include people who have visited or interacted with animals brought from African regions (10-12). For instance, human contact with dogs that had come into contact with African rodents was linked to the more than 70 cases of MPX detected in the U.S. in 2003. In a similar vein, seven instances of MPX were reported in the UK between 2018 and 2022, four of which involved people who had returned from African nations (5,13). An international outbreak of MPX began in 2022. The WHO was notified of the first occurrences in May 2022. Then, the number of afflicted people rose quickly. A significant number of the initial cases were detected in people who had attended a large LGBT + gathering in the Spanish Canary Islands. The disease rapidly spread across several European nations as a result of this incident. However, through close personal contact, MPX eventually spread locally in many nations (14-17).
Morphology and Pathogenesis of Monkeypox Virus
The mature virion of MPX has a unique and complex structure. A dumbbell-shaped double-stranded DNA genome comprises the viral core. All of the genetic information required for viral survival and replication within the host cell is encoded in this genome. In addition to 30 membrane-bound and structural viral proteins, MPX virions contain vital enzymes needed for genome replication, including DNA-dependent RNA polymerase that the virus encodes. The genome of the virus consists of 197, 000 base pairs. Inverted terminal repeats, essential for genome packaging and replication, are present in its structure. Furthermore, there are over 190 non-overlapping open reading frames in the genome. The assembly of full virions and the replication of the virus depend on at least 90 of these open reading frames (18,19).
The nose, mouth, and skin are the three possible entry points for the MPXV, which can then multiply there. The virus then travels to nearby lymph nodes and can potentially spread to other organs afterward (20,21). MPXV is an exception to the rule that most DNA viruses replicate in the cell nucleus, instead choosing to do so in the cytoplasm. Its replication depends on particular proteins (19).
Endocytosis and membrane fusion are two ways in which MPXV might enter cells. Furthermore, the two varieties of MPXV have different envelopes and surface proteins that affect how the virus enters and exits cells. Additionally, compared to strains found in West Africa, MPXV strains detected in Central Africa typically induce a more severe illness (21).
The host cell’s cytoplasm is where immature virions (IMVs) are created following DNA replication, transcription, and translation. IMVs can mature into enveloped virions (EEVs), which are transported by microtubules to the cell surface and then released. Occasionally, the infected cell may lyse and release the virions. Some EEVs have the ability to transform into cell-associated EEVs once they attach to the cell surface. These virions can use actin filaments to move to adjacent cells (22,23).
Such a cytokine storm can develop in the most serious manifestations of MPX viral infection as an overwhelming inflammatory event. Available evidence indicates that the response against MPX could involve both type 1 T helper (Th1) and Th2 varieties; under certain conditions, a more pronounced Th2 response might overshadow the Th1 response. The Th2 response, for instance, is characterized by the secretion of various cytokines, including interleukin-4 (IL-4), IL-5, and IL-6, which are important for humoral immunity and inflammation. Similarly, increased levels of the anti-inflammatory cytokine IL-10 have also been observed, which may be implicated in the downregulation of the Th1 response that is equally essential in intracellular pathogen responses, such as viruses. On the other hand, Th1-associated pro-inflammatory cytokines, such as tumor necrosis factor-α, interferon-gamma, and IL-2, would typically be low in these instances, reflecting the type of shift in immune balance. This shift in immune responses may play an important role in the severity of the disease and the incidence of complications such as organ failure in severe cases. Prior infection with MPX has once again proven to lead an individual to respond in a more regulated manner during subsequently occurring infections (24).
Clinical Manifestations and Monkeypox Virus Diagnosis
Clinically, smallpox and MPX are comparable viruses. This disease typically takes 7–14 days to incubate in humans, although it can take anywhere from 4 to 21 days (2).
A brief febrile phase (averaging 8 days) precedes MPX. In addition to a fever, individuals may experience headaches, backaches, and muscle aches during this period. They can feel weakness, exhaustion, and perspiration. A rash can develop on any region of the body, including the face, lips, hands, feet, chest, genital area, anus, and even the area surrounding the eyes, following this brief fever period, which typically lasts one to three days. The lesions on the skin begin as flat macules and then grow into small papules. Small blisters emerge as a result of the clear fluid that fills these bumps. These blisters eventually evolve into pus-filled pimples as the fluid inside them becomes cloudy and yellow. These acne lesions ultimately dry up, crust over, and heal when the crusts fall off. At this point, the individual is no longer able to spread the illness to other individuals. Severe MPX is more common in those with compromised immune systems. The most frequent side effect of this illness is scarring at the site of skin lesions. Research has, however, demonstrated the possibility of more severe side effects, including encephalitis, pneumonia, respiratory issues, and eye infections. Untreated eye infections can lead to corneal ulcers and even blindness (Figure 2) (2,11,14,20,25-28).
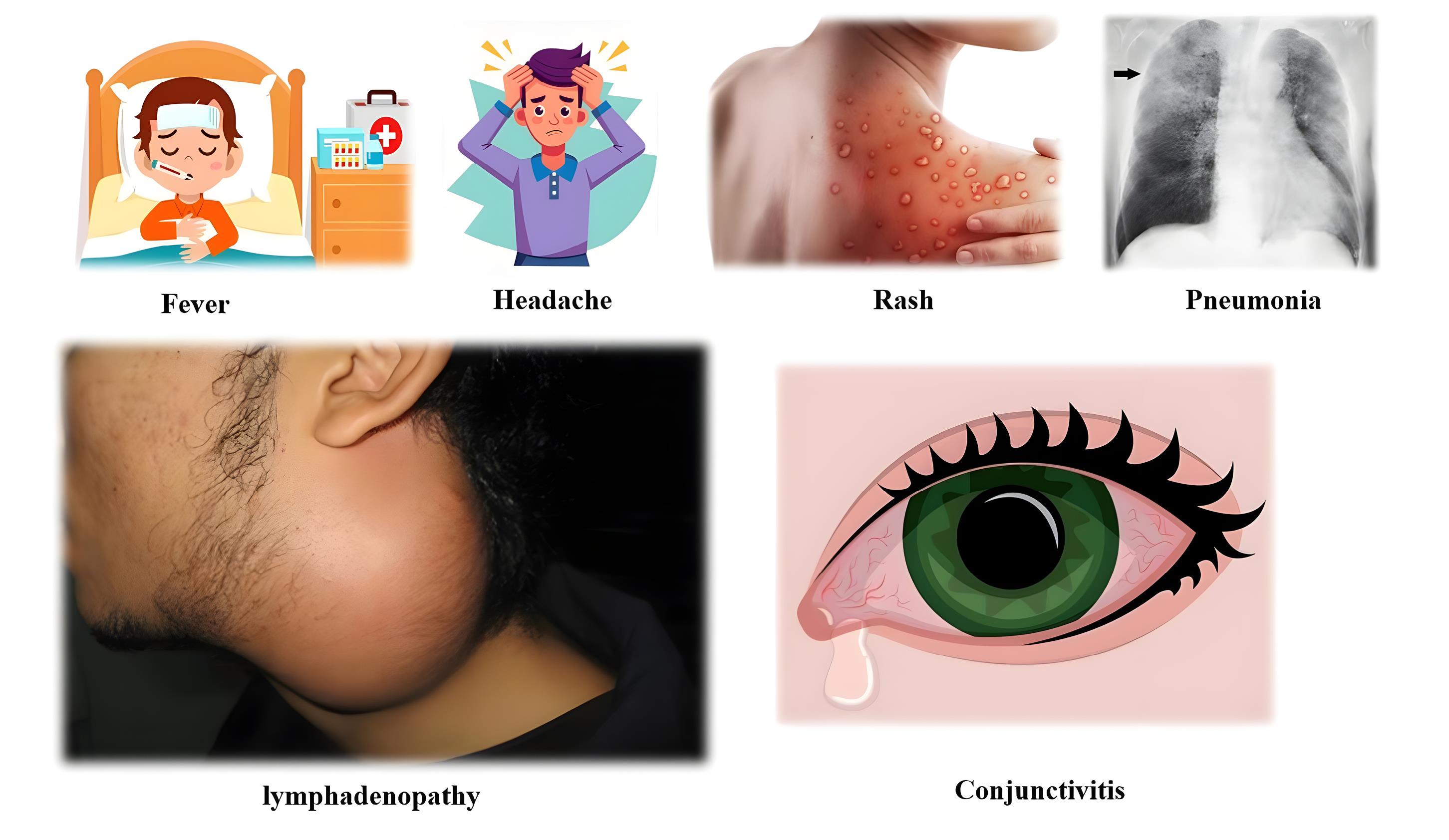
Figure 2.
Important Signs and Symptoms of Monkeypox
.
Important Signs and Symptoms of Monkeypox
Despite the apparent similarities between smallpox and MPX, a crucial clinical indicator for distinguishing between the two illnesses is lymphadenopathy, which is present in 90% of MPX cases. Swollen lymph nodes in the neck, groin, and beneath the chin are some of the most important indicators that differentiate MPX from related skin conditions, such as smallpox and chickenpox (Figure 2) (29).
MPX can lead to severe gastrointestinal issues, including vomiting and diarrhea, in addition to skin lesions. These symptoms may cause dehydration, low blood protein (albumin), and nutritional problems. These individuals may occasionally require intravenous infusions due to fluid and nutritional loss (29).
A precise diagnosis of MPX is necessary for choosing the best course of therapy and preventing the infection from spreading, as the clinical symptoms of smallpox, chickenpox, and MPX are extremely similar. We need to be aware of the subtle variations in the clinical manifestations of smallpox, chickenpox, syphilis, and chancroid to differentiate MPX from these related illnesses. Electron microscopy can also be useful in this context (30).
Although clinical indicators can aid in distinguishing MPX from other skin conditions, a conclusive diagnosis necessitates specific laboratory tests, such as enzyme-linked immunosorbent assay (ELISA), serology, and others, which are discussed in detail in the following section (2,30).
Using immunohistochemical staining, it is possible to distinguish between infections caused by the varicella-zoster virus (VZV) and herpes simplex viruses (HSV-1 and HSV-2). Certain antibodies do not react with HSV or VZV, but they can specifically detect the MPXV. Similarly, some antibodies only recognize the VZV and HSV viruses instead of reacting to the MPXV. Furthermore, some antibodies assist in the diagnosis of MPX by identifying specific antigens of the virus (30).
Certain immunoglobulinM and G antibodies can be found in the blood of MPX patients using ELISA. Usually, 5–8 days following infection, these antibodies begin to appear in the blood. However, this test may yield false positives due to cross-reactivity between the antigens of the MPXV and other poxviruses. Moreover, considering that the virions of the MPXV are morphologically identical, diagnosing the infection with electron microscopy is not always possible (18,20).
A number of techniques, including polymerase chain reaction (PCR), reverse transcription PCR, loop-mediated isothermal amplification, recombinase polymerase amplification, and restriction fragment length polymorphism, are commonly used in the molecular diagnosis of MPX. These techniques utilize specific viral genes as markers to aid in identifying the virus. These methods often aim to amplify the genes PRO18, B6R, E9L, and several other genes (18,31).
Monkeypox Virus Therapy
There is currently no approved medication for the complete recovery from MPX. Nonetheless, this illness typically resolves on its own with little to no intervention. As a result, most current treatments focus on managing and alleviating the patient’s symptoms. The primary course of treatment for MPX is supportive care, which may include medications to treat secondary bacterial infections and reduce fever and pain. However, some individuals may require more extensive treatment, including those with weakened immune systems, expectant mothers, and children (32).
Even though MPX can be extremely dangerous, managing symptoms is now the main focus of treatment. To address this illness, researchers are seeking novel medications. Given the many similarities between smallpox and MPX, researchers have explored antiviral medication used for smallpox to treat MPX. These research findings suggest that effective therapies for MPX may soon be developed. Medications such as cidofovir, brincidofovir, and tecovirimat are often used by researchers to investigate and treat orthopoxvirus infections (33), the details of which are presented in Table 1.
Table 1.
An Overview of Antiviral Medications Authorized by the FDA and Their Mechanism of Action in Blocking the MPXV
|
Drug Therapy
|
FDA Approval Status
|
Mechanism of Action
|
References
|
| Cidofovir |
Yes (CMV) |
Preventing the replication of viral DNA by inhibiting viral DNA polymerase |
(34) |
| Tecovirimat |
Yes (Smallpox) |
Inhibiting the production of infectious virus particles by blocking the viral protein VP37 |
(34) |
| Brincidofovir |
Yes (Smallpox) |
Functioning as a prodrug that inhibits viral DNA polymerase after being transformed into cidofovir |
(34) |
Note. FDA: The U.S. Food and Drug Administration; MPXV: Monkeypox virus; CMV: Cytomegalovirus.
Tecovirimat can be obtained as an injectable or as an oral capsule containing 200 mg. The Centers for Disease Control states that this medication is authorized for use in treating MPX in the U.S. Antiviral medications such as cidofovir and brincidofovir can be utilized as well. The U.S. Food and Drug Administration has approved these medications for the treatment of smallpox and cytomegalovirus infections (32).
Immunoglobulins have been demonstrated in numerous studies to be highly effective against viruses. Consequently, many viral infections are currently being treated with this particular therapeutic approach. Immunoglobulins are frequently utilized in the injection of rabies immunoglobulin for individuals who have been bitten by dogs (35).
Intravenous vaccinia immunoglobulin (VIGIV) has been licensed by the U.S. Food and Drug Administration for managing smallpox vaccination-related issues. Furthermore, a protocol for using VIGIV in treating illnesses such as MPX has been proposed by the Centers for Disease Control. Nevertheless, further research is needed to determine how effectively this medication treats MPX. As a result, not all individuals with MPX should use this medication. Nonetheless, the use of VIGIV might be recommended for individuals with compromised immune systems who have been exposed to the illness (36).
It is crucial to precisely identify the specific components of the virus (antigens) that activate the immune system (immunogens) in order to utilize antibodies in the treatment or prevention of viral illnesses. This comprehensive knowledge is still lacking in the case of the smallpox virus and its close relatives, such as the MPX virus. However, research has indicated that the body may be somewhat protected against severe MPX disease by antibodies produced against the IMV (L1R) portion of the virus. According to another research report, a combination of various IMV and EEV virus components (L1R, A27L, A33R, and B5R) can significantly enhance protection against this illness. These findings suggest that these viral components may serve as excellent targets for the development of novel vaccines and antibodies that provide defense against MPX and other closely related viruses (35).
Prevention and Vaccination of Monkeypox Virus
Control techniques (e.g., avoiding contact with infected hosts, cleaning surfaces, isolating sick patients, using protective gear when providing patient care, fully cooking food, and engaging in safe sexual behavior) are advised to stop the spread of the MPXV (33,37).
The management of MPX includes raising public awareness, educating the public, assessing the effectiveness of vaccinations, and implementing hygienic controls to contain sick animals. The effectiveness of vaccination in preventing and controlling the disease is being investigated through ongoing clinical trials. Important control techniques include quarantining contaminated animals and implementing targeted immunization programs for high-risk groups (38).
Smallpox, cowpox, vaccinia, and MPXV are part of the Poxviridae family of viruses, which share numerous genetic and antigenic similarities. Due to these parallels, vaccination against one of these viruses or infection with another can protect against other members of the same family (39).
The smallpox vaccine (Vaccinia) can reduce cases of severe MPX by around 85% and significantly prevent smallpox and MPX. However, at the moment, there is not enough vaccine. This vaccination comes in two primary varieties (MVA and ACAM2000). As a second-generation vaccine, the MVA vaccine has demonstrated robust immunogenicity and a good safety profile across various groups, including those with weakened immune systems. In contrast, due to the possibility of more serious side effects, the ACAM2000 vaccine is used less frequently. While both vaccines have the capacity to elicit potent immune responses, there are differences regarding their administration and safety and how long it takes for an immune response to develop (40,41).
Prioritizing vaccination for high-risk groups, such as healthcare workers, immunocompromised individuals, and children, is crucial due to the limited supply of vaccines. These populations face a higher risk of severe illness and death, which is why they receive priority. MVA is recommended for pregnant women because of the potential dangers associated with live vaccinations. While pre-exposure vaccination is effective, post-exposure vaccination can also be administered promptly (within four days). Furthermore, ring vaccination-vaccinating those in close contact with patients-can be highly beneficial for epidemic control, along with quick diagnosis and patient quarantine (41,42).
Challenges and Future Research Directions
The recent outbreak of the COVID-19 has caused numerous concerns for the government and healthcare providers. The recent outbreak of MPX in areas where it is not endemic underscores the importance of being prepared for the unexpected. Infection control relies on the early and accurate diagnosis of the illness, but this has been compromised by misdiagnosis and varying clinical presentations in different geographical areas (43,44). Regarding direct healthcare costs (hospitalization, doctor visits, medical supplies and drugs, and quarantine), a significant portion of the financial burden caused by a viral pandemic is spent here (45). Fears, misinformation, negative social stigmas, and cultural discrepancies all primarily contribute to why individuals receive no immunizations or medical care. Furthermore, in poorer countries, doctors, due to a lack of training and know-how, may not recognize serious signs of disease or prescribe the necessary medication (46).
The MPX pandemic requires new and targeted therapies. Researchers are attempting to find treatments that specifically target the chemicals responsible for its spread. Biomarkers can serve as indicators to help pinpoint these drugs and develop even stronger medicines. Furthermore, due to the close relationship between smallpox and MPX, understanding smallpox pathophysiology could lead to new therapies for MPX (33).
The clinical similarities between smallpox and MPX, although genetically distinct, have allowed for the creation of new antiviral therapies. Researchers are working to discover new biomarkers for MPX that might serve as targets for therapy. For example, there is the protein interferon-gamma and a compound called thymidine kinase that have been found in many studies to be associated with both diseases. If these biomarkers are targeted, drugs can be developed that directly alter the pathogenic mechanisms of the virus. In other words, the study of smallpox can lead to a better understanding of MPX and therefore more specific and effective treatments for this disease (33,47). Nanotechnology provides innovative approaches to the synthesis of antiviral medications by modifying the characteristics of materials at a very small scale. Studies have demonstrated that by disrupting the viral replication cycle and strengthening the immune system, silver nanoparticles (NPs) can effectively treat illnesses such as MPX. Research findings indicate that silver NPs can stop the spread of viruses by attaching to infected cells and interfering with the metabolic processes of the virus, even though the precise mechanism of action of these particles is not entirely understood yet. In light of these discoveries, it is anticipated that silver NPs and other comparable NPs will be crucial in the future for managing viral infections (33,48).
The most pivotal first step in addressing viral challenges, such as MPX, would be to create the next generation of vaccines based on advanced technologies and platforms. Furthermore, mRNA vaccines, which have performed exceptionally well in the case of COVID-19, are promising in terms of fast, flexible, and efficient development for a wide range of diseases, including poxviruses. These vaccines assist the body against the virus by encoding viral proteins that alert the immune system to the presence of the virus. In addition, there is active research on DNA vaccines and vaccines using viral vectors that could elicit stronger immune responses and longer-lasting immunity. The development of a pan-poxvirus vaccine that could provide protection against a wide range of poxvirus families is important, as it will prevent the emergence of new diseases caused by this viral family. Additionally, significant development potential exists for vaccine adjuvants that could enhance and prolong protective immune responses, substantially increasing vaccine efficacy. Furthermore, studies related to the longevity of vaccine protection and the need for booster shots would be critical in achieving effective vaccination programs (49).
In addition to vaccine development, there are also innovative public health initiatives designed specifically to mitigate outbreaks, such as that of MPX. It is essential to implement more complex surveillance and early detection systems, including cutting-edge technologies such as wastewater surveillance for viral outbreaks in communities. The development of rapid and accurate point-of-care testing has been shown to facilitate quick diagnostics and the implementation of appropriate control measures. The use of smartphones can enhance disease transmission control through improved contact tracing and isolation measures. Moreover, enhancing public participation and control of disease outbreaks includes the rollout of well-crafted ‘vaccine’ and misinformation countering public awareness campaigns that are evidence-based and strategic. The other key elements of public health strategies entail the formulation of stockpiles of vaccines and antiviral agents in readiness for potential epidemics, along with proper mechanisms for the equitable distribution of vaccines, especially in low-income countries (50).
Past pandemics have led to great advances in biotechnology, increased funding for infectious disease control, and significant upgrades to surveillance systems. The public health system can better prepare for the future, though with improved control measures, more research, and more comprehensive studies on various aspects of MPX (43). While several treatments for MPX exist, it is unknown how well they work in general. To determine the best approach, the National Institutes of Health (NIH) is conducting a clinical trial (51). However, the emergence of these viral diseases has focused attention on the need for improved laboratory practices, more robust disease surveillance networks, a fuller understanding of how viruses interact with the human body, and the development of rapid diagnostic tools (52). By making significant research investments and investing in new technology, it is possible to create efficient plans for stopping and managing future epidemics (43,53).
Conclusion
A new viral disease called MPX has suddenly swept across the globe and has become a serious health issue. This disease is characterized by many symptoms, including fever, headache, muscle pain, and skin lesions. The signs and symptoms of this disease resemble those of other skin diseases, and therefore specific testing (PCR and ELISA) is necessary for a proper diagnosis. These assays, which recognize the virus genome in clinical specimens, assist in accurate diagnosis. There is no single surefire drug to cure MPX. Some medications (e.g., tecovirimat and cidofovir) are used to treat other viral infections but can also be utilized to treat MPX. More research is needed to determine the effectiveness of these drugs. Some immunity to MPX exists from the smallpox vaccinations, which were used to eradicate smallpox. However, with the smallpox outbreak, these vaccinations have become harder to obtain due to a lack of production. Since there are no definitive diagnoses or cures, the development of safer vaccines, the implementation of comprehensive health precautions, and the strengthening of surveillance systems should be a high priority in containing this disease. To effectively combat MPX and other emerging infectious diseases, a One Health approach must be applied-one that recognizes the complex interplay between humans, animals, and the environment. Global health is being threatened by MPX. Establishing comprehensive health programs, funding research and development, and encouraging international collaboration are all imperative to effectively combat this disease. A combined approach can assist us in fighting this disease and preventing widespread epidemics.
Acknowledgments
We would like to thank all those who contributed to this study.
Competing Interests
The authors declare that they have no conflict of interests.
Ethical Approval
Not applicable.
Funding
This manuscript received no financial assistance, grant, or sponsorship from any authors.
References
- Letafati A, Sakhavarz T. Monkeypox virus: a review. Microb Pathog 2023; 176:106027. doi: 10.1016/j.micpath.2023.106027 [Crossref] [ Google Scholar]
- Altindis M, Puca E, Shapo L. Diagnosis of monkeypox virus - an overview. Travel Med Infect Dis 2022; 50:102459. doi: 10.1016/j.tmaid.2022.102459 [Crossref] [ Google Scholar]
- León-Figueroa DA, Bonilla-Aldana DK, Pachar M, Romaní L, Saldaña-Cumpa HM, Anchay-Zuloeta C. The never-ending global emergence of viral zoonoses after COVID-19? The rising concern of monkeypox in Europe, North America and beyond. Travel Med Infect Dis 2022; 49:102362. doi: 10.1016/j.tmaid.2022.102362 [Crossref] [ Google Scholar]
- Karagoz A, Tombuloglu H, Alsaeed M, Tombuloglu G, AlRubaish AA, Mahmoud A. Monkeypox (mpox) virus: classification, origin, transmission, genome organization, antiviral drugs, and molecular diagnosis. J Infect Public Health 2023; 16(4):531-41. doi: 10.1016/j.jiph.2023.02.003 [Crossref] [ Google Scholar]
- Mitjà O, Ogoina D, Titanji BK, Galvan C, Muyembe JJ, Marks M. Monkeypox. Lancet 2023; 401(10370):60-74. doi: 10.1016/s0140-6736(22)02075-x [Crossref] [ Google Scholar]
- Yinka-Ogunleye A, Aruna O, Dalhat M, Ogoina D, McCollum A, Disu Y. Outbreak of human monkeypox in Nigeria in 2017-18: a clinical and epidemiological report. Lancet Infect Dis 2019; 19(8):872-9. doi: 10.1016/s1473-3099(19)30294-4 [Crossref] [ Google Scholar]
- Bunge EM, Hoet B, Chen L, Lienert F, Weidenthaler H, Baer LR. The changing epidemiology of human monkeypox-a potential threat? A systematic review. PLoS Negl Trop Dis 2022; 16(2):e0010141. doi: 10.1371/journal.pntd.0010141 [Crossref] [ Google Scholar]
- Soheili M, Nasseri S, Afraie M, Khateri S, Moradi Y, Mahdavi Mortazavi SM. Monkeypox: virology, pathophysiology, clinical characteristics, epidemiology, vaccines, diagnosis, and treatments. J Pharm Pharm Sci 2022; 25:297-322. doi: 10.18433/jpps33138 [Crossref] [ Google Scholar]
- Ihekweazu C, Yinka-Ogunleye A, Lule S, Ibrahim A. Importance of epidemiological research of monkeypox: is incidence increasing?. Expert Rev Anti Infect Ther 2020; 18(5):389-92. doi: 10.1080/14787210.2020.1735361 [Crossref] [ Google Scholar]
- Vaughan A, Aarons E, Astbury J, Balasegaram S, Beadsworth M, Beck CR. Two cases of monkeypox imported to the United Kingdom, September 2018. Euro Surveill 2018; 23(38):1800509. doi: 10.2807/1560-7917.Es.2018.23.38.1800509 [Crossref] [ Google Scholar]
- Vaughan A, Aarons E, Astbury J, Brooks T, Chand M, Flegg P. Human-to-Human Transmission of Monkeypox Virus, United Kingdom, October 2018. Emerg Infect Dis 2020; 26(4):782-5. doi: 10.3201/eid2604.191164 [Crossref] [ Google Scholar]
- Yong SE, Ng OT, Ho ZJM, Mak TM, Marimuthu K, Vasoo S. Imported monkeypox, Singapore. Emerg Infect Dis 2020; 26(8):1826-30. doi: 10.3201/eid2608.191387 [Crossref] [ Google Scholar]
- Zachary KC, Shenoy ES. Monkeypox transmission following exposure in healthcare facilities in nonendemic settings: low risk but limited literature. Infect Control Hosp Epidemiol 2022; 43(7):920-4. doi: 10.1017/ice.2022.152 [Crossref] [ Google Scholar]
- Antinori A, Mazzotta V, Vita S, Carletti F, Tacconi D, Lapini LE. Epidemiological, clinical and virological characteristics of four cases of monkeypox support transmission through sexual contact, Italy, May 2022. Euro Surveill 2022; 27(22):2200421. doi: 10.2807/1560-7917.Es.2022.27.22.2200421 [Crossref] [ Google Scholar]
- Iñigo Martínez J, Gil Montalbán E, Jiménez Bueno S, Martín Martínez F, Nieto Juliá A, Sánchez Díaz J. Monkeypox outbreak predominantly affecting men who have sex with men, Madrid, Spain, 26 April to 16 June 2022. Euro Surveill 2022; 27(27):2200471. doi: 10.2807/1560-7917.Es.2022.27.27.2200471 [Crossref] [ Google Scholar]
- Perez Duque M, Ribeiro S, Martins JV, Casaca P, Leite PP, Tavares M. Ongoing monkeypox virus outbreak, Portugal, 29 April to 23 May 2022. Euro Surveill 2022; 27(22):2200424. doi: 10.2807/1560-7917.Es.2022.27.22.2200424 [Crossref] [ Google Scholar]
- Selb R, Werber D, Falkenhorst G, Steffen G, Lachmann R, Ruscher C. A shift from travel-associated cases to autochthonous transmission with Berlin as epicentre of the monkeypox outbreak in Germany, May to June 2022. Euro Surveill 2022; 27(27):2200499. doi: 10.2807/1560-7917.Es.2022.27.27.2200499 [Crossref] [ Google Scholar]
- Anwar F, Haider F, Khan S, Ahmad I, Ahmed N, Imran M. Clinical manifestation, transmission, pathogenesis, and diagnosis of monkeypox virus: a comprehensive review. Life (Basel) 2023; 13(2):522. doi: 10.3390/life13020522 [Crossref] [ Google Scholar]
- Kugelman JR, Johnston SC, Mulembakani PM, Kisalu N, Lee MS, Koroleva G. Genomic variability of monkeypox virus among humans, Democratic Republic of the Congo. Emerg Infect Dis 2014; 20(2):232-9. doi: 10.3201/eid2002.130118 [Crossref] [ Google Scholar]
- Alakunle E, Moens U, Nchinda G, Okeke MI. Monkeypox virus in Nigeria: infection biology, epidemiology, and evolution. Viruses 2020; 12(11):1257. doi: 10.3390/v12111257 [Crossref] [ Google Scholar]
- Saied AA, Dhawan M, Metwally AA, Fahrni ML, Choudhary P, Choudhary OP. Disease history, pathogenesis, diagnostics, and therapeutics for human monkeypox disease: a comprehensive review. Vaccines (Basel) 2022; 10(12):2091. doi: 10.3390/vaccines10122091 [Crossref] [ Google Scholar]
- Cifuentes-Munoz N, El Najjar F, Dutch RE. Viral cell-to-cell spread: conventional and non-conventional ways. Adv Virus Res 2020; 108:85-125. doi: 10.1016/bs.aivir.2020.09.002 [Crossref] [ Google Scholar]
- Kumar N, Acharya A, Gendelman HE, Byrareddy SN. The 2022 outbreak and the pathobiology of the monkeypox virus. J Autoimmun 2022; 131:102855. doi: 10.1016/j.jaut.2022.102855 [Crossref] [ Google Scholar]
- Johnston SC, Johnson JC, Stonier SW, Lin KL, Kisalu NK, Hensley LE. Cytokine modulation correlates with severity of monkeypox disease in humans. J Clin Virol 2015; 63:42-5. doi: 10.1016/j.jcv.2014.12.001 [Crossref] [ Google Scholar]
- Abdelaal A, Serhan HA, Mahmoud MA, Rodriguez-Morales AJ, Sah R. Ophthalmic manifestations of monkeypox virus. Eye (Lond) 2023; 37(3):383-5. doi: 10.1038/s41433-022-02195-z [Crossref] [ Google Scholar]
- McCollum AM, Damon IK. Human monkeypox. Clin Infect Dis 2014; 58(2):260-7. doi: 10.1093/cid/cit703 [Crossref] [ Google Scholar]
- Petersen E, Kantele A, Koopmans M, Asogun D, Yinka-Ogunleye A, Ihekweazu C. Human monkeypox: epidemiologic and clinical characteristics, diagnosis, and prevention. Infect Dis Clin North Am 2019; 33(4):1027-43. doi: 10.1016/j.idc.2019.03.001 [Crossref] [ Google Scholar]
- Zambrano PG, Acosta-España JD, Mosquera Moyano F, Altamirano Jara JB. Sexually or intimately transmitted infections: a look at the current outbreak of monkeypox in 2022. Travel Med Infect Dis 2022; 49:102383. doi: 10.1016/j.tmaid.2022.102383 [Crossref] [ Google Scholar]
- Niu L, Liang D, Ling Q, Zhang J, Li Z, Zhang D. Insights into monkeypox pathophysiology, global prevalence, clinical manifestation and treatments. Front Immunol 2023; 14:1132250. doi: 10.3389/fimmu.2023.1132250 [Crossref] [ Google Scholar]
- Zahmatyar M, Fazlollahi A, Motamedi A, Zolfi M, Seyedi F, Nejadghaderi SA. Human monkeypox: history, presentations, transmission, epidemiology, diagnosis, treatment, and prevention. Front Med (Lausanne) 2023; 10:1157670. doi: 10.3389/fmed.2023.1157670 [Crossref] [ Google Scholar]
- Gong Q, Wang C, Chuai X, Chiu S. Monkeypox virus: a re-emergent threat to humans. Virol Sin 2022; 37(4):477-82. doi: 10.1016/j.virs.2022.07.006 [Crossref] [ Google Scholar]
- Cheema AY, Ogedegbe OJ, Munir M, Alugba G, Ojo TK. Monkeypox: a review of clinical features, diagnosis, and treatment. Cureus 2022; 14(7):e26756. doi: 10.7759/cureus.26756 [Crossref] [ Google Scholar]
- Upadhayay S, Arthur R, Soni D, Yadav P, Navik U, Singh R. Monkeypox infection: the past, present, and future. Int Immunopharmacol 2022; 113(Pt A):109382. doi: 10.1016/j.intimp.2022.109382 [Crossref] [ Google Scholar]
- Kumar P, Chaudhary B, Yadav N, Devi S, Pareek A, Alla S. Recent advances in research and management of human monkeypox virus: an emerging global health threat. Viruses 2023; 15(4):937. doi: 10.3390/v15040937 [Crossref] [ Google Scholar]
- Ghaseminia M. Preventing monkeypox outbreaks: focus on diagnosis, care, treatment, and vaccination. J Clin Transl Sci 2023; 7(1):e60. doi: 10.1017/cts.2023.11 [Crossref] [ Google Scholar]
- O’Shea J, Filardo TD, Morris SB, Weiser J, Petersen B, Brooks JT. Interim guidance for prevention and treatment of monkeypox in persons with HIV infection - United States, August 2022. MMWR Morb Mortal Wkly Rep 2022; 71(32):1023-8. doi: 10.15585/mmwr.mm7132e4 [Crossref] [ Google Scholar]
- Varela K, Brown JA, Lipton B, Dunn J, Stanek D, Behravesh CB. A review of zoonotic disease threats to pet owners: a compendium of measures to prevent zoonotic diseases associated with non-traditional pets: rodents and other small mammals, reptiles, amphibians, backyard poultry, and other selected animals. Vector Borne Zoonotic Dis 2022; 22(6):303-60. doi: 10.1089/vbz.2022.0022 [Crossref] [ Google Scholar]
- Awan UA, Riasat S, Naeem W, Kamran S, Khattak AA, Khan S. Monkeypox: a new threat at our doorstep!. J Infect 2022; 85(2):e47-8. doi: 10.1016/j.jinf.2022.05.027 [Crossref] [ Google Scholar]
- Hirani R, Noruzi K, Iqbal A, Hussaini AS, Khan RA, Harutyunyan A. A review of the past, present, and future of the monkeypox virus: challenges, opportunities, and lessons from COVID-19 for global health security. Microorganisms 2023; 11(11):2713. doi: 10.3390/microorganisms11112713 [Crossref] [ Google Scholar]
- Petersen BW, Kabamba J, McCollum AM, Lushima RS, Wemakoy EO, Muyembe Tamfum JJ. Vaccinating against monkeypox in the Democratic Republic of the Congo. Antiviral Res 2019; 162:171-7. doi: 10.1016/j.antiviral.2018.11.004 [Crossref] [ Google Scholar]
- See KC. Vaccination for monkeypox virus infection in humans: a review of key considerations. Vaccines (Basel) 2022; 10(8):1342. doi: 10.3390/vaccines10081342 [Crossref] [ Google Scholar]
- Mohanty B, Costantino V, Narain J, Chughtai AA, Das A, MacIntyre CR. Modelling the impact of a smallpox attack in India and influence of disease control measures. BMJ Open 2020; 10(12):e038480. doi: 10.1136/bmjopen-2020-038480 [Crossref] [ Google Scholar]
- Hamdana AH, Mohsin H, Habib Tharwani Z, Masood W, Furqana AQ, Sohail A. Monkeypox virus and other emerging outbreaks: an overview and future perspective. Inquiry 2023; 60:469580231175437. doi: 10.1177/00469580231175437 [Crossref] [ Google Scholar]
- Ogoina D, Iroezindu M, James HI, Oladokun R, Yinka-Ogunleye A, Wakama P. Clinical course and outcome of human monkeypox in Nigeria. Clin Infect Dis 2020; 71(8):e210-4. doi: 10.1093/cid/ciaa143 [Crossref] [ Google Scholar]
- Rasmussen MK, Kronborg C, Fasterholdt I, Kidholm K. Economic evaluations of interventions against viral pandemics: a scoping review. Public Health 2022; 208:72-9. doi: 10.1016/j.puhe.2022.05.001 [Crossref] [ Google Scholar]
- Reynolds MG, McCollum AM, Nguete B, Shongo Lushima R, Petersen BW. Improving the care and treatment of monkeypox patients in low-resource settings: applying evidence from contemporary biomedical and smallpox biodefense research. Viruses 2017; 9(12):380. doi: 10.3390/v9120380 [Crossref] [ Google Scholar]
- Rodrigues Garcia D, Rodrigues de Souza F, Paula Guimarães A, Castro Ramalho T, Palermo de Aguiar A, Celmar Costa França T. Design of inhibitors of thymidylate kinase from Variola virus as new selective drugs against smallpox: part II. J Biomol Struct Dyn 2019; 37(17):4569-79. doi: 10.1080/07391102.2018.1554510 [Crossref] [ Google Scholar]
- Rai M, Deshmukh SD, Ingle AP, Gupta IR, Galdiero M, Galdiero S. Metal nanoparticles: the protective nanoshield against virus infection. Crit Rev Microbiol 2016; 42(1):46-56. doi: 10.3109/1040841x.2013.879849 [Crossref] [ Google Scholar]
- Sang Y, Zhang Z, Liu F, Lu H, Yu C, Sun H. Monkeypox virus quadrivalent mRNA vaccine induces immune response and protects against vaccinia virus. Signal Transduct Target Ther 2023; 8(1):172. doi: 10.1038/s41392-023-01432-5 [Crossref] [ Google Scholar]
- Morgan O, Redies I, Leiva Rioja ZB, Brownstein J, George D, Golding J. Innovations in public health surveillance: updates from a forum convened by the WHO Hub for Pandemic and Epidemic Intelligence, 2 and 3 February 2022. Euro Surveill 2022; 27(15):2200302. doi: 10.2807/1560-7917.Es.2022.27.15.2200302 [Crossref] [ Google Scholar]
- Sherwat A, Brooks JT, Birnkrant D, Kim P. Tecovirimat and the treatment of monkeypox - past, present, and future considerations. N Engl J Med 2022; 387(7):579-81. doi: 10.1056/NEJMp2210125 [Crossref] [ Google Scholar]
- Khalil AT, Ali M, Tanveer F, Ovais M, Idrees M, Shinwari ZK. Emerging viral infections in Pakistan: issues, concerns, and future prospects. Health Secur 2017; 15(3):268-81. doi: 10.1089/hs.2016.0072 [Crossref] [ Google Scholar]
- Graham BS, Sullivan NJ. Emerging viral diseases from a vaccinology perspective: preparing for the next pandemic. Nat Immunol 2018; 19(1):20-8. doi: 10.1038/s41590-017-0007-9 [Crossref] [ Google Scholar]