Avicenna Journal of Clinical Microbiology and Infection. 11(3):136-140.
doi: 10.34172/ajcmi.3540
Original Article
Nosocomial Infection Reporting System Improvement in the Public Hospitals
Mahnaz Hadipour 1  , Narges Tavakolilia 2, Elham Feizabad 1, Mojtaba Sedaghat 1, Seyyed Farshad Allameh 1, Ali Ganjali Khan 1, Arash Seyfi 3, Mehrdad Ahmadi 1, Zainab Siami 1, Aziz Rasouli 1, *
, Narges Tavakolilia 2, Elham Feizabad 1, Mojtaba Sedaghat 1, Seyyed Farshad Allameh 1, Ali Ganjali Khan 1, Arash Seyfi 3, Mehrdad Ahmadi 1, Zainab Siami 1, Aziz Rasouli 1, *
Author information:
1Vice-Chancellor for Treatment Affairs, Tehran University of Medical Sciences, Tehran, Iran
2Family Health Department, Vice-Chancellor for Health Affairs, Tehran University of Medical Sciences, Tehran, Iran
3Infectious Diseases Department, Research Center for Antibiotics Stewardship and Antimicrobial Resistance, Tehran University of Medical Sciences, Tehran, Iran
Abstract
Background: The nosocomial infection (NI) rate in developing countries is about 20–25%. However, in Iran, this is nearly 2.95%, which may be related to an incorrect and incomplete reporting system. Hence, the present study aimed at investigating NI reporting challenges in hospitals affiliated with Tehran University of Medical Sciences (TUMS) and providing solutions for its improvement.
Methods: This interventional study was conducted on 14 public hospitals affiliated with TUMS. The study population included all nurses and doctors of the infection control team of the hospitals. As an intervention, a training workshop was held for the selected hospital infection control teams. The other intervention was the standardization of NI indicators in the National NI Surveillance System (NNISS). Before and after the intervention, the infection control teams of the TUMS vice-chancellor for treatment affairs assessed the hospitals regarding NI reporting. All analyses were performed using SPSS version 26 software at a significant level of less than 0.05.
Results: The results of the present study showed that the rate of NIs reported in the hospitals has grown significantly in consecutive years, indicating 2.98%, 2.81%, 3.62%, and 4.41%, respectively, from 2014 to 2017. The correct syntax of patients with a positive culture, changes in the type of antibiotics, wound changes, and NI symptoms were 100%, 43.6%, 33.3%, and 31.25%, respectively.
Conclusion: The findings related to hospital infections were close to what was expected, and it is expected that more significant improvements will be experienced with more control and supervision in the field of diagnosis and how to analyze hospital infections.
Keywords: Nosocomial infections, Improvement, Solutions
Copyright and License Information
© 2024 The Author(s); Published by Hamadan University of Medical Sciences.
This is an open-access article distributed under the terms of the Creative Commons Attribution License (
https://creativecommons.org/licenses/by/4.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Please cite this article as follows: Hadipour M, Tavakolilia N, Feizabad E, Sedaghat M, Allameh SF, Ganjali Khan A, et al. Nosocomial infection reporting system improvement in the public hospitals. Avicenna J Clin Microbiol Infect. 2024; 11(3):136-140. doi:10.34172/ajcmi.3540
Introduction
Nosocomial infections (NIs) have always been one of the major hospital problems, increasing the duration of a patient’s stay, morbidity and mortality, as well as hospital costs (1).
Globally, more than 1.4 million people suffer from hospital infections per year in developing and developed countries. According to reports, the hospital infection incidence is nearly 5%–10% and more than 25% in developed and some developing countries, respectively (2,3).
It must be considered that more than 70% of hospital infections include urinary tract infections, pneumonia, bloodstream infections, and surgical site infections (4).
Bacteria are the most common microorganisms that cause hospital infections. Bacteria (e.g., coagulase-negative Staphylococci, Staphylococcus aureus, Streptococcus species, Klebsiella pneumonia, Klebsiella oxytoca, and Escherichia coli),viruses (e.g., hepatitis B and Candhuman deficiency virus), fungi (e.g., Candida species and Aspergillus fumigatus), and parasites have caused hospital epidemics in 71%, 21%, 5%, and 3% of cases, respectively; however, the cause of infection has not been identified in 2% of the cases (5,6).
The National NI Surveillance System (NNISS) is one of the best sources of data gathering about hospital infections (7-9). According to NNISS, the most important causes of hospital infections are aerobic bacteria (87%), anaerobic bacteria (3%), fungi (9%), and other types of viruses and parasites (1%). In general, among the types of hospital infections, Escherichia coli is the most common pathogen, followed by S. aureus (5,10).
The NI rate in developing countries is about 20%–25%. However, in Iran, this rate is nearly 2.95%, which is probably associated with an incomplete and incorrect reporting system (11).
Hence, the present study seeks to investigate the NI reporting challenges in hospitals affiliated with Tehran University of Medical Sciences (TUMS) and then provide solutions for its improvement.
Materials and Methods
This before-after interventional study was conducted on 14 public hospitals affiliated with TUMS from 2014 to 2021. The study population included all doctors and nurses of the infection control team of the hospitals.
NIs are considered any systemic or localized infections (confirmed clinically or with laboratory tests) occurring 48 hours after admission and including urinary tract infections, bloodstream infections, surgical site infections, and ventilator-associated pneumonia (12,13).
As an intervention, a training workshop was held for the selected hospital infection control teams (nurses and doctors). This workshop had two main topics, namely, the correct diagnosis and reporting of four main NIs and the way to enter the related data into the NNIS of the hospitals.
The other intervention was the standardization of NI indicators in the NNIS. In this regard, the denominator of the fraction was changed from 24-hour patient hospitalization to the patient’s day.
Before and after the intervention, the infection control teams of the TUMS Vice-Chancellor for Treatment Affairs assessed the hospitals in terms of NI reporting. This evaluation was performed through field visits, medical record reviews, and hospital information system evaluation (for comprehensive antibiotics orders). All analyses were conducted using SPSS software (version 26) at a significant level of less than 0.05.
Results
The results revealed that the rate of NIs reported in the hospitals has significantly increased in consecutive years, demonstrating 2.98%, 2.81%, 3.62%, and 4.41%, respectively, from 2014 to 2017. The hospital infection rate was 6.78%, on average, during the 15 months of 2020-2021 (Figure 1).
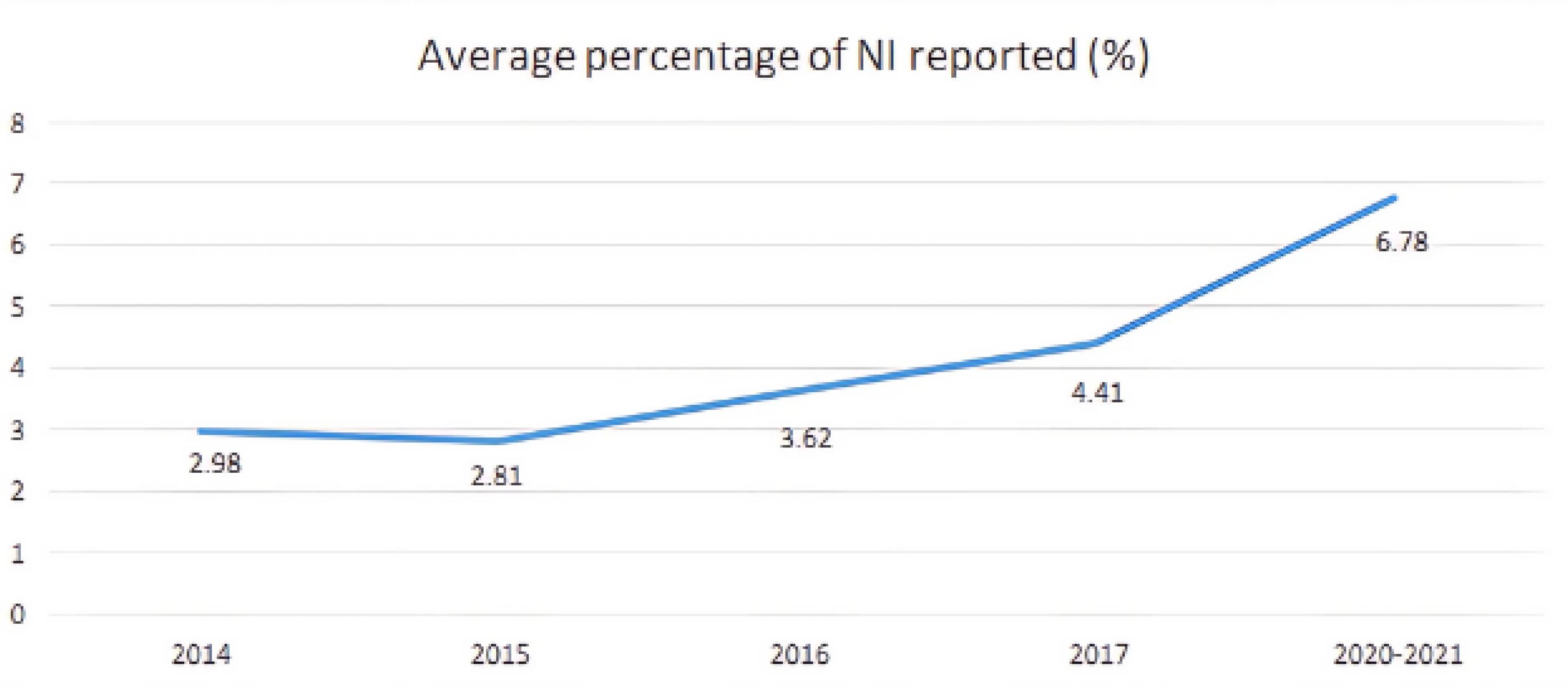
Figure 1.
Average Results of Nosocomial Infections by Year of Investigation in Hospitals Covered by Tehran University of Medical Sciences
.
Average Results of Nosocomial Infections by Year of Investigation in Hospitals Covered by Tehran University of Medical Sciences
The correct syntax of patients with positive culture was 100%, and changes in the type of antibiotics, wound changes, and NI symptoms were 43.6%, 33.3%, and 31.25%, respectively.
Table 1 presents the average NI separately for each type of infection in hospitals covered by TUMS during the 15 months of 2020 and 2021.
Table 1.
Average Nosocomial Infections Separately for Each Type of Infection in Hospitals Covered by Tehran University of Medical Sciences (2020–2021)
|
Hospital
|
Ventilator-Associated Pneumonia
|
Urinary Tract Infection
|
Bloodstream Infection
|
Surgical Site Infection
|
| A |
0.47 |
0.76 |
1.92 |
1.23 |
| B |
3.13 |
4.71 |
2.18 |
1.13 |
| C |
0 |
0.79 |
1.02 |
1.19 |
| D |
0 |
0.95 |
0.49 |
6.51 |
| E |
0 |
0.16 |
0 |
0 |
| F |
2.53 |
1.94 |
1.8 |
1.43 |
| G |
0.02 |
2.35 |
6.03 |
1.35 |
| H |
0.12 |
1.88 |
1.46 |
3.28 |
| I |
0 |
0 |
0 |
1.95 |
| J |
2.26 |
2.66 |
2.47 |
1.56 |
| K |
0.1 |
0.22 |
1.42 |
1.67 |
| L |
0 |
1.09 |
1.97 |
0.48 |
| M |
0.37 |
0.94 |
1.17 |
1.22 |
| N |
0 |
0.06 |
0.04 |
2.09 |
Discussion
In a descriptive-analytical study conducted on all hospitalized patients under 15 years of age with the standard method of the hospital infection care system, the overall rate of hospital infection was estimated at 8.5% (14).
NIs are those infections that are caused by medical care and are considered undesirable results in patients who need care. NIs are becoming increasingly more important and seriously challenge the health systems of the countries (15).
NIs have always been one of the major health and treatment problems at the same time as the expansion of hospitals, and increasing the duration of the patient’s stay in the hospital causes an increase in the number of infections and deaths from these infections, and as a result, increases the hospital costs (15,16).
The point of view regarding low reporting of hospital infection can hide the need to improve the quality of services, especially at the level of clinical services of the hospital. The research conducted in the state of Victoria also showed that managers tend to estimate the hospital infection rate lower than the actual rate (17).
Considering that more than 70% of hospital infections are of urinary, surgical, respiratory, and blood types, the data related to these four infections have been examined in the first stage of establishing the hospital infection care system in the country. This interventional study was conducted in hospitals covered by TUMS in 2018 and for one year to diagnose, track, and report hospital infections for four common hospital infections.
Hospitals had problems filling statistics in NNIS software; thus, a training workshop was held for infection control supervisors, and then hospitals were checked for reporting statistics (18).
The results demonstrated that the correct performance of hospitals in relation to the items of how to report was 31.25%. In addition, the correct reporting rate of positive culture, the rate of reporting wound changes, the rate of correct reporting of antibiotic changes, and the rate of correct reporting of fever in these hospitals were 100%, 33.33%, 43.75%, and 37.5%, respectively. Due to the modification of the software, the modification of the denominator of the fractions, and the placement of the day patient and the day tool instead of 24-hour hospitalization, it was possible to compare the infection percentage of hospitals with expected numbers (19,20).
The prevalence of hospital infection recorded in many hospitals of the country indicates the concealment of cases of infection because, based on internal and external evidence, the actual prevalence of hospital infection in the country is estimated to be between 8% and 10%, and its occurrence in hospitals is undeniable (21). Fortunately, with the corrective measures taken regarding the reporting of NIs in the present study, a significant increase was observed in the reporting of NIs in hospitals covered by the TUMS, which confirms the success of this project and the improvement of the reporting process (20,21).
One of the four effective factors in the effectiveness of the infection control program is the presence of a knowledgeable infection control doctor or nurse who plays an active role in the infection control program (22). The underreporting of hospital infections can be prevented when all components of the care system play an active role. At the head of them are infection control doctors and nurses. Improving the knowledge of infection control doctors and nurses is an important factor that can lead to the improvement of hospital infection reporting (23).
Van Jamet found that despite their good knowledge, most of the studied doctors and nurses had problems in accessing, understanding, applying, and accepting the hospital infection control program (24). In this research, by holding explanatory and educational classes in the field of NIs for infection control doctors and nurses of all the hospitals implementing the project, it was attempted to update the information of these people to have the greatest impact on their interventions. Financial incentives were also used in this field (23,25).
Disease detection was improved with monthly control and monitoring. In addition, reforms were made in the hospital and university infection control committee to intervene and correctly report the diagnosis and analyze the hospital infection index. Further, the hospitals were obliged to examine the hospital infection statistics in the form of a run chart (26). Then, each hospital was compared and evaluated with itself, and according to the expected limit of single-specialty and general hospitals, a report card was issued for each hospital in terms of NIs (27,28).
Considering that the NI reporting system in the country’s hospitals has problems and there are few real reports, there is a need for a fundamental revision of the NI reporting system in all hospitals of the country (29). It is possible to take appropriate measures and interventions to control hospital infections when the report of the hospital infection care system is correct and accurate (30,31). Thus, the current research can be used as a suitable model in this regard.
One of the most important strengths of the current research was the active participation of all people involved in the process of reporting hospital infections, as well as the full support of the senior officials of the hospitals and vice-chancellors of TUMS, which led to the success of this project.
On the other hand, one of the most important limitations of this research was the reluctance of a number of relevant personnel, especially hospital nurses, to report timely and correct NIs, who attempted to solve this problem to some extent by justifying them.
Conclusion
Overall, the findings related to hospital infections were close to what was expected, and it is expected that further essential improvements in more control and supervision be observed in the field of diagnosis and the way to analyze hospital infections. In Iran, the existence of a system to perform targeted corrective interventions is absolutely necessary. Unfortunately, the performance of the hospital infection control system in our country is only focused on collecting the statistics of the hospital infection rate. Fortunately, the current research revealed that problems related to the actual reporting of hospital infections can be reduced to a large extent by performing necessary and expert interventions at different levels of the process of recording and reporting hospital infections.
Authors’ Contribution
Conceptualization: Seyyed Farshad Allameh.
Data curation: Arash Seifi, Mehrdad Ahmadi.
Formal analysis: Mojtaba Sedaghat.
Funding acquisition: Ali Ganjali Khan.
Investigation: Mahnaz Hadipour.
Methodology: Mojtaba Sedaghat.
Project administration: Zainab Siami.
Supervision: Aziz Rasouli.
Writing–original draft: Elham Feizabad, Narges Tavakolilia.
Writing–review & editing: Mahnaz Hadipour, Aziz Rasouli.
Competing Interests
None declared.
Ethical Approval
This study received ethical approval from the Institutional Review Board of TUMS (IR.TUMS.MEDICINE.REC.1400.150) based on the Declaration of Helsinki.
Funding
This study was supported by the Vice-Chancellor for Treatment Affairs of TUMS.
References
- Raoofi S, Pashazadeh Kan F, Rafiei S, Hosseinipalangi Z, Noorani Mejareh Z, Khani S. Global prevalence of nosocomial infection: a systematic review and meta-analysis. PLoS One 2023; 18(1):e0274248. doi: 10.1371/journal.pone.0274248 [Crossref] [ Google Scholar]
- Masoumi Asl H, Zahraei SM, Majidpur A, Nateghian A, Afhami S, Rahbar M, et al. National Guideline of Nosocomial Infections Surveillance. Ministry of Health & Medical Education; 2005. p. 111-40.
- Saavedra CH, Ordóñez KM, Díaz JA. [Nosocomial infections impact in a hospital in Bogota, Colombia: effects on mortality and hospital costs]. Rev Chilena Infectol 2015; 32(1):25-9. doi: 10.4067/s0716-10182015000200006.[Spanish] [Crossref] [ Google Scholar]
- Zahraei SM, Eshrati B, Masoumi Asl H, Pezeshki Z. Epidemiology of four main nosocomial infections in Iran during March 2007 - March 2008 based on the findings of a routine surveillance system. Arch Iran Med 2012; 15(12):764-6. [ Google Scholar]
- Brannigan ET, Murray E, Holmes A. Where does infection control fit into a hospital management structure?. J Hosp Infect 2009; 73(4):392-6. doi: 10.1016/j.jhin.2009.03.031 [Crossref] [ Google Scholar]
- Nouri F, Karami P, Zarei O, Kosari F, Alikhani MY, Zandkarimi E. Prevalence of common nosocomial infections and evaluation of antibiotic resistance patterns in patients with secondary infections in Hamadan, Iran. Infect Drug Resist 2020; 13:2365-74. doi: 10.2147/idr.S259252 [Crossref] [ Google Scholar]
- Farr BM. Reasons for noncompliance with infection control guidelines. Infect Control Hosp Epidemiol 2000; 21(6):411-6. doi: 10.1086/501783 [Crossref] [ Google Scholar]
- Curtis A, Moore Z, Patton D, O’Connor T, Nugent L. Does using a cellular mobile phone increase the risk of nosocomial infections in the neonatal intensive care unit: a systematic review. J Neonatal Nurs 2018; 24(5):247-52. doi: 10.1016/j.jnn.2018.05.008 [Crossref] [ Google Scholar]
- Faraji Hormozi S, Saeedi AA, Aminianfar M, Salmani Alishah M, Darvishi M. Studying the frequency of nosocomial infection and its relative factors in the intensive care unit of hospitals based upon NNI system. Eurasian J Anal Chem 2018; 13(3):em16. doi: 10.20933/ejac/85014 [Crossref] [ Google Scholar]
- Reid R, Sheehy C, Jabbour L. Risk factors and interventions against nosocomial infections across multiple African countries: a systematic review. CPQ Medicine 2018; 2(2):1-12. [ Google Scholar]
- Bagheri P, Rezaei F, Roodgari A, Rokhsari M, Fararouei M. Nosocomial infections in an Iranian educational hospital: an evaluation study of the Iranian nosocomial infection surveillance system. BMC Infect Dis 2021; 21(1):1256. doi: 10.1186/s12879-021-06948-1 [Crossref] [ Google Scholar]
- Kouchak F, Askarian M. Nosocomial infections: the definition criteria. Iran J Med Sci 2012; 37(2):72-3. [ Google Scholar]
- Boev C, Kiss E. Hospital-acquired infections: current trends and prevention. Crit Care Nurs Clin North Am 2017; 29(1):51-65. doi: 10.1016/j.cnc.2016.09.012 [Crossref] [ Google Scholar]
- Masoumi Asl H. Epidemiologic Evaluation of Nosocomial Infections in Patients Under 15 Years Old by NNIS Standard Methods in Rasool Akram Hospital [dissertation]. Tehran: Tehran University of Medical Science; 2002.
- Griemsmann M, Tergast TL, Simon N, Kabbani AR, Manns MP, Wedemeyer H. Nosocomial infections in female compared with male patients with decompensated liver cirrhosis. Sci Rep 2022; 12(1):3285. doi: 10.1038/s41598-022-07084-9 [Crossref] [ Google Scholar]
- Aghdassi SJ, Hansen S, Bischoff P, Behnke M, Gastmeier P. A national survey on the implementation of key infection prevention and control structures in German hospitals: results from 736 hospitals conducting the WHO Infection Prevention and Control Assessment Framework (IPCAF). Antimicrob Resist Infect Control 2019; 8:73. doi: 10.1186/s13756-019-0532-4 [Crossref] [ Google Scholar]
- Carter M, Cohen C, Murphy C, Wecke A, Collopy B, MacLeod A, et al. Report of the Expert Working Group on Surveillance of Nosocomial Infections. Acute Health Division, Quality and Care Continuity Branch Victorian Government Department of Human Services, Melbourne Victoria; 2002. p. 19-20.
- Biscetti L, Cameriere V, Rossi T, Potente E, Sabbatini D, Bollettini F. Dementia, stroke, age, use of medical devices and antipsychotic drugs may increase the risk of nosocomial infections among elderly patients hospitalized at neurology clinics. Sci Rep 2023; 13(1):18687. doi: 10.1038/s41598-023-46102-2 [Crossref] [ Google Scholar]
- Stiller A, Salm F, Bischoff P, Gastmeier P. Relationship between hospital ward design and healthcare-associated infection rates: a systematic review and meta-analysis. Antimicrob Resist Infect Control 2016; 5:51. doi: 10.1186/s13756-016-0152-1 [Crossref] [ Google Scholar]
- Ssekitoleko RT, Oshabaheebwa S, Munabi IG, Tusabe MS, Namayega C, Ngabirano BA. The role of medical equipment in the spread of nosocomial infections: a cross-sectional study in four tertiary public health facilities in Uganda. BMC Public Health 2020; 20(1):1561. doi: 10.1186/s12889-020-09662-w [Crossref] [ Google Scholar]
- Emami Razavi H. Nosocomial Infections Surveillance. Iran: Ministry of Health & Medical Education, Deputy of Curative Affairs; 2009.
- Shojaee H, Shirani SH. Preface of Principal, Epidemiology & Control of Hospital Infections. Isfahan: Isfahan University of Medical Sciences Publication; 2003. p. 40.
- Guggenbichler JP, Assadian O, Boeswald M, Kramer A. Incidence and clinical implication of nosocomial infections associated with implantable biomaterials - catheters, ventilator-associated pneumonia, urinary tract infections. GMS Krankenhhyg Interdiszip 2011; 6(1):Doc18. doi: 10.3205/dgkh000175 [Crossref] [ Google Scholar]
- van Gemert-Pijnen J, Hendrix MG, van der Palen J, Schellens PJ. Performance of methicillin-resistant Staphylococcus aureus protocols in Dutch hospitals. Am J Infect Control 2005; 33(7):377-84. doi: 10.1016/j.ajic.2004.10.009 [Crossref] [ Google Scholar]
- Fürnkranz U, Walochnik J. Nosocomial infections: do not forget the parasites!. Pathogens 2021; 10(2):238. doi: 10.3390/pathogens10020238 [Crossref] [ Google Scholar]
- Yadollahi M, Kashkooe A, Feyzi M, Bornapour S. Risk factors of mortality in nosocomial infected traumatic patients in a trauma referral center in south of Iran. Chin J Traumatol 2018; 21(5):267-72. doi: 10.1016/j.cjtee.2018.03.002 [Crossref] [ Google Scholar]
- De Cock AM, Strens D, Van Osta P, Standaert B. Infections and hospital bed-days among aging adults: a five-year retrospective study in a Belgian general hospital. Front Med Technol 2022; 4:912469. doi: 10.3389/fmedt.2022.912469 [Crossref] [ Google Scholar]
-
Rosenthal VD. Device-associated nosocomial infections in limited-resources countries: findings of the International Nosocomial Infection Control Consortium (INICC). Am J Infect Control 2008;36(10):S171.e7-S171.e12. doi: 10.1016/j.ajic.2008.10.009.
- Corley A, Lye I, Lavana JD, Ahuja A, Anstey CM, Jarrett P. Nosocomial infection prevalence in patients undergoing extracorporeal membrane oxygenation (ECMO): protocol for a point prevalence study across Australia and New Zealand. BMJ Open 2019; 9(7):e029293. doi: 10.1136/bmjopen-2019-029293 [Crossref] [ Google Scholar]
- Wolkewitz M, Cooper BS, Palomar-Martinez M, Alvarez-Lerma F, Olaechea-Astigarraga P, Barnett AG. Multilevel competing risk models to evaluate the risk of nosocomial infection. Crit Care 2014; 18(2):R64. doi: 10.1186/cc13821 [Crossref] [ Google Scholar]
- Aktar F, Tekin R, Güneş A, Ülgen C, Tan İ, Ertuğrul S. Determining the independent risk factors and mortality rate of nosocomial infections in pediatric patients. Biomed Res Int 2016; 2016:7240864. doi: 10.1155/2016/7240864 [Crossref] [ Google Scholar]