Avicenna Journal of Clinical Microbiology and Infection. 10(1):27-31.
doi: 10.34172/ajcmi.2023.5454
Original Article
Target Population, Targeted Health Education: A Case-Based Reasoning Proposed for the Control of Human Hydatidosis
Zainab Sadeghi Dehkordi 1, *  , Hamidreza Moslemimanesh 1, Ali Sadeghi-Nasab 2
, Hamidreza Moslemimanesh 1, Ali Sadeghi-Nasab 2
Author information:
1Department of Pathobiology, Faculty of Veterinary Science, Bu-Ali Sina University, Hamedan, Iran
2Department of Clinical Science, Faculty of Veterinary Science, Bu-Ali Sina University, Hamedan Iran
Abstract
Background: Cystic echinococcosis (CE), caused by Echinococcus granulosus sensu lato, is a common zoonotic disease in Iran. Identifying various risk factors of this disease can pave the way for launching control and prevention programs, as well as special health education for target populations. For this purpose, this retrospective study investigated the demographic characteristics and risk factors of human hydatidosis in Hamedan.
Methods: The registered demographic characteristics of 98 patients, the risk factors of echinococcosis transmission, and the involved organs were analyzed through the profile form of patients who underwent CE surgery in two main hospitals of Hamedan province during 2014-2018. Data were analyzed using the chi-square test (or Fisher’s exact test), independent t-test, and one-way analysis of variance with Stata 16 software at a significance level of α≥0.05.
Results: Forty-eight (48.97%) and 50 (51.02%) cases of the 98 registered CE surgeries were females and males, respectively. The age range of the patients was 8-91 years, with the significantly highest rate in 21-30 years old (23.46%, P<0.05). In addition, 77.78% of urban residents reported contact with contaminated vegetables vs. 58.49% of infected rural reported contact with contaminated vegetables and/ or dogs (P<0.05). The prevalence of infection merely in the liver (60.20%) was significantly higher than in the other organs (P<0.05).
Conclusion: According to the results, it seems that the targeted health education should be focused on people in their third decade of life and younger. Further, the education of urban residents should be focused more on the health of vegetables and villagers based on the simultaneous explanation of the dangers of contaminated vegetables and dogs.
Keywords: Echinococcus granulosus, Hamedan, Hospital records, Risk factors
Copyright and License Information
© 2023 The Author(s); Published by Hamadan University of Medical Sciences.
This is an open-access article distributed under the terms of the Creative Commons Attribution License (
http://creativecommons.org/licenses/by/4.0), which permits unrestricted use, distribution, and reproduction in any medium provided the original work is properly cited.
Please cite this article as follows: Sadeghi Dehkordi Z, Moslemimanesh H, Sadeghi-Nasab A. Target population, targeted health education: a case-based reasoning proposed for the control of human hydatidosis. Avicenna J Clin Microbiol Infect. 2023; 10(1):27- 31. doi:10.34172/ajcmi.2023.5454
Introduction
Human cystic echinococcosis (CE) is caused by the larval stage of Echinococcus granulosus. It is one of the most common zoonotic parasitic infections, globally, especially in endemic and hyper-endemic areas with a widespread distribution in the Mediterranean region and Asian countries (1). In Iran, hydatidosis is an endemic zoonotic disease with extensive impacts on the country’s economy and public health (2). Dogs and canines are the definitive hosts and humans, and other animals act as intermediate. Carnivores are infected by ingesting contaminated viscera, and humans become infected by ingesting eggs in the environment, direct contact with infected canines, and consumption of contaminated food or water (3).
In humans, hydatid cysts are commonly found in the liver and lungs although it has also been reported in other organs such as the brain (4), heart (5), bones and spine (6), breast (7), eye (8), ovary and fallopian tube (9), and parathyroid gland (10). Previous studies in Iran have reported that the prevalence of the disease has been relatively high in Mashhad, Kashan, Arak, Yasouj, Babol, and Yazd (11-17). In human patients, the surgical removal of cysts is the choice of treatment in many cases. It imposes a fundamental burden on human life and public health worldwide. Studies have shown that hydatidosis is responsible for 1% of surgical treatment cases in Iran, and the human rate of infection is 0.6-1.2% (18).
Moreover, environmental and cultural conditions, various hosts, and human individuals’ behaviors and social characteristics have already changed the prevalence pattern, transmission, and distribution of parasitic diseases (15). Hamedan province is a potential area for hydatid cyst infection due to the variety of climate zones, the presence of stray dogs, and pasture-based animal husbandry. Hamedan livestock is more traditional farming (19,20). Additionally, there have been very limited studies on the prevalence and frequency of human hydatidosis in Hamedan (19,21). Therefore, the spread of the infectious disease can be controlled using an awareness schedule of the epidemic status of the disease in the region and considering the effective risk factors. For this purpose, hospital data and records are remarkable, and a vast variety of sources are used to assess the epidemiology and distinct feature of the disease. Accordingly, this case-based study was conducted to review again the demographic-geographical aspects, risk factors, and the distribution of parasitic tissue in humans in 2014-2018 in Hamedan province, Iran.
Materials and Methods
In a retrospective case-based analysis, the demographic characteristics of hydatid cyst patients who were candidates for surgery, as well as the place of residence (rural or urban), the involved organs, and based on a history questionnaire, when admitted to the hospital, and the possible mode of infection transmission (contact with dogs and/or contaminated vegetables), were investigated from 2014 to 2018. The registered cases included 48 female and 50 male patients in the age range of 8-91 years who were referred to two main hospitals in Hamedan. The data were analyzed by chi-square (or Fisher’s exact test), independent t-test, and one-way analysis of variance (ANOVA) using Stata 16 software at a significance level of α ≤ 0.05.
Results
Out of a total of 98 CE cases, 48 cases (48.97%) were females and 50 cases (51.03%) were males.The prevalence of infection in villagers was slightly higher than that of urban residents, and the possible route of infection is partly blamed on contaminated vegetables (Tables 1 and 2). The youngest and oldest male patients were 8 and 91 years old, respectively. In general, in females and males, the highest rate of infection occurred in the third decade of life (29.17%) and the third and fourth decades (20.00%) of life, respectively. The infection rate in patients under ten years old and over 70 years old was significantly lower than in other groups (Table 3).
Table 1.
Prevalence and Age Distribution of Registered Patients Based on Gender, Place of Residence, and Route of Infection (n = 98)
|
|
Gender
|
Residence
|
Route of Infection
|
|
Female (n=48)
|
Male (n=50)
|
Rural (n=53)
|
Urban (n=45)
|
Veg (n=57)
|
Veg+Dog (n=41)
|
| Prevalence, (%) |
48.97 (39.12-58.90) |
51.03 (41.09-60.87) |
54.08 (44.06-63.78) |
45.91 (36.21-55.93) |
58.16 (48.02-67.65) |
41.83 (32.34-51.97) |
| Agea, Mean ± SD |
37.62 ± 17.15 |
39.2 ± 19.37 |
40.11 ± 19.26 |
36.44 ± 16.96 |
39.21 ± 18.71 |
37.34 ± 17.74 |
|
P value |
0.67 |
0.32 |
0.62 |
Note. SD: Standard deviation; Veg: Probably contaminated vegetables; Veg + Dog: Probably contaminated vegetables or contact with dogs.
a Independent t test.
Table 2.
Prevalence and Distribution of Registered Patients Based on Gender, Place of Residence and Route of Infection (n = 98)
|
|
Female
|
Male
|
Total
|
|
Rural
|
Urban
|
Rural
|
Urban
|
Rural
|
Urban
|
| Veg |
10 (37.04) |
17 (62.96) |
12 (46.15) |
14 (53.85) |
22 (41.51) |
31 (55.49) |
| Veg + Dog |
19 (90.48) |
2 (9.52) |
16 (66.67) |
8 (33.33) |
35 (77.78) |
10 (22.22) |
|
P value |
0.000a |
0.144b |
0.000b |
Note. Numbers in parentheses represent percentages; Veg: Probably contaminated vegetables; Veg + Dog: Contaminated vegetables or contact with dogs.
a Chi-square; b Fisher’s exact test.
Table 3.
Gender and Age Prevalence of Registered Hydatid Cyst Infection (n = 98)
|
Age (y)
|
Female
|
Male
|
Total
|
| ≤ 10 |
2.08 (0.29-13.65) |
10.00 (4.18-22.07) |
6.12 (2.73-13.13) |
| 1 |
5 |
6 |
| 11-20 |
12.50 (5.67-25.36) |
6.00 (1.92-17.23) |
9.18 (4.79-16.88) |
| 6 |
3 |
9 |
| 21-30 |
29.17 (17.98-43.61) |
18.00 (9.56-31.31) |
23.46 (16.00-33.03) |
| 14 |
9 |
23 |
| 31-40 |
16.67 (8.49-30.14) |
20.00 (11.03-33.52) |
18.36 (11.79-27.46) |
| 8 |
10 |
18 |
| 41-50 |
10.42 (4.35-22.90) |
20.00 (11.03-33.52) |
15.30 (9.35-24.03) |
| 5 |
10 |
15 |
| 51-60 |
14.58 (7.05-27.77) |
12.00 (5.44-24.44) |
13.26 (7.78-21.69) |
| 7 |
6 |
13 |
| 61-70 |
10.42 (4.35-22.90) |
6.00 (1.92-17.23) |
8.16 (4.08-15.65) |
| 5 |
3 |
8 |
| ≥ 71 |
4.17 (1.03-15.42) |
8.00 (3.0019.66) |
6.12(2.73-13.13) |
| 2 |
4 |
6 |
| Total |
48.97 (39.12-58.90) |
51.03 (41.09-60.87) |
- |
| 48 |
50 |
98 |
Note. Odd rows: Percentage (95% confidence interval); Even rows: Numbers.
Furthermore, there was a significant difference in gender, place of residence, and the route of infection (P ≤ 0.05). In this regard, 77.78% of the urban patients were infected due to the consumption of contaminated vegetables, while 58.4% of rural patients were infected via contaminated vegetables and contact with dogs. Further, 90.48% of rural females claimed that they were simultaneously in direct contact with the dogs and contaminated vegetables, while 62.96% of urban females were infected via contaminated vegetables (P ≤ 0.000). In contrast, no association was found between the infection rate in rural and urban males and both routes (P = 0.144).
Additionally, the highest prevalence of infection was significantly reported in the liver (60.2%, P ≤ 0.05). The other involved organs are listed in Table 4. Moreover, no significant difference was observed between the involved organs and age of patients (P = 0.079).
Table 4.
Frequency of Tissue Distribution of Hydatid Cyst and its Relationship With Age
|
|
n
|
Percentage (CI 95%)
|
Age (Mean±SD)
|
| Liver |
59 |
60.20 (50.11-69.50) |
41.05 ± 18.94 |
| Lung |
14 |
14.29 (8.59-22.81) |
28.50 ± 11.65 |
| Liver and Lung |
11 |
11.22 (6.28-19.26) |
31.55 ± 20.95 |
| Coelom |
6 |
6.12 (2.75-13.08) |
38.50 ± 14.45 |
| Others |
8 |
8.16 (4.10-15.60) |
45.88 ± 14.79 |
|
P value |
< 0.05 |
0.079a |
Note. CI: Confidence interval; SD: Standard deviation; Others: Spleen, Kidney, Bone, Femur, Liver + Stomach + Eye, Liver + Kidney, Liver + Spleen + Eye, Liver + Lung + Coelom each including 1 case (n = 8). a One-way analysis of variance.
According to the different residential areas of Hamedan province, the highest and lowest rates of reported hydatidosis belonged to Melayer (41.83%) and Faminin (1.02%), respectively (Figure 1).
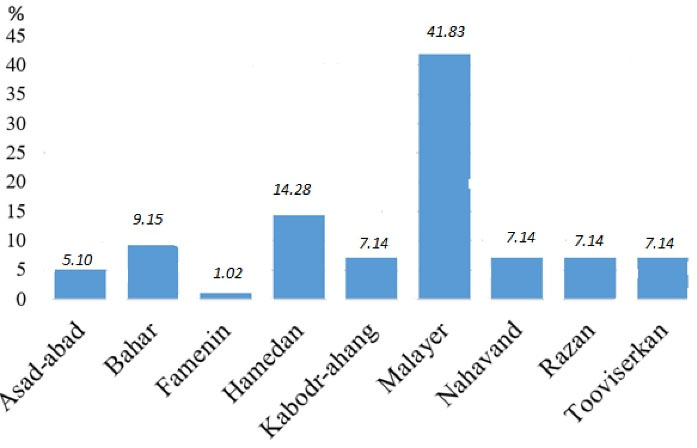
Figure 1.
The Prevalence of the CE Disease in Different Areas of Hamedan Province.
Note. CE: Cystic echinococcosis. The prevalence of the disease in Malayerr has been significantly higher than in the other areas (P < 0.05 ).
.
The Prevalence of the CE Disease in Different Areas of Hamedan Province.
Note. CE: Cystic echinococcosis. The prevalence of the disease in Malayerr has been significantly higher than in the other areas (P < 0.05 ).
The highest frequency of the cases was recorded 31.98, 31.63% in 2014 and lowest frequency was reported 7.98: 7.14% in 2017 (Figure 2).
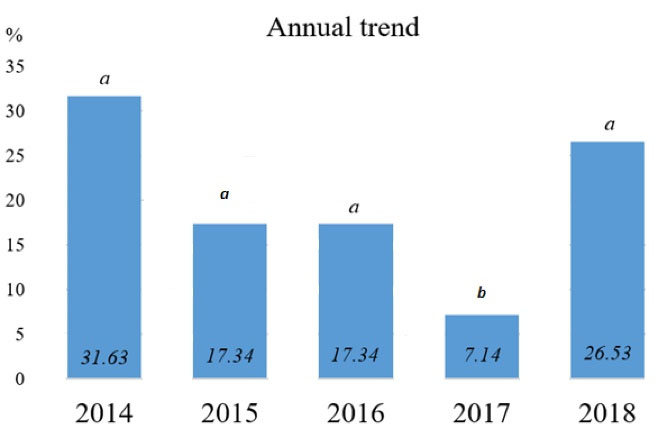
Figure 2.
Annual Trend of Cystic Echinococcosis in Hamedan Province During 2014-2018. Note. The same letters indicate no significant difference in the prevalence of infection in different years (P < 0.05 )
.
Annual Trend of Cystic Echinococcosis in Hamedan Province During 2014-2018. Note. The same letters indicate no significant difference in the prevalence of infection in different years (P < 0.05 )
Discussion
In this study, the hospital records of CE patients were 98 in Hamedan from 2014 to 2018. Out of 48 infected women, 27 cases were from rural areas and 21 cases were from urban areas, and this ratio for 50 infected men was 26 versus 24, respectively. The infection rate and age did not represent a significant difference based on gender, place of residence, and possible route of infection (Table 2). This finding can result in the same susceptibility of both genders and probably infection transmission through direct and/or indirect contact with contaminated sources. Obviously, the most important finding was a significant age trend which was focused on the third decade for females, while it was described on the third, fourth, and fifth decades for males (Table 3). For this reason, a high probability of exposure to influential risk factors and even age-specific trends can theoretically have an impact on this event. In this way, there is no scientific explanation for the latter, and it comes to mind only as a possible hypothesis. Overall, the young patients who are of working age are more exposed to contaminated sources which can be one of the most common probable hypotheses.
Considerably, 77.78% of urban patients reported the consumption of contaminated vegetables, while 58.4% of rural patients were infected via contaminated vegetables and/or contact with dogs. However, 90.48% of rural females claimed that they were simultaneously in direct contact with the dogs and/or contaminated vegetables, whereas 62.96% of urban females were infected via contaminated vegetables (P ≤ 0.000). Nonetheless, there was no remarkable difference between the routes of infestation of rural and urban males (P = 0.144, Table 2). Several reasons could clarify this finding. For instance, the low health literacy level of rural women can be pointed out as the cause of consuming contaminated vegetables (22). In addition, household activities and rural women’s contact with other livestock are traditionally a part of their daily routine life. Hence, education and training strategies for rural and urban females should be established in different subjects. Previous studies mentioned that rural women have the highest chance of contact with the infection sources such as dogs, soil, and vegetables because women are often a vital resource in the agriculture and rural economy. This finding is in line with those of prior studies in Iran and Iraq (12,13,17,18,23). On the other hand, since dogs are more frequent in rural than urban settings, researchers have indicated it as an important risk factor for CE infection worldwide (24,25). Further, antiparasitic treatments are not often acceptable for the herd and guard dogs in rural areas. Conventionally, the slaughtered infected viscera of ruminants are commonly considered food for dogs (20,22). On the other hand, wild canines are nearby rural areas and can probably pass the egg parasite (3). Thus, training of the mentioned points is imperative for rural people (Table 2). Moreover, large numbers of stray dogs in rural areas are one of the major risk factors for their roaming freely and contaminating vegetables due to dropping feces containing eggs (22,26,27).
It is considerable that the majority of the organs involved in CE cases were merely the liver [59 out of 98: (60.2%)] and lunge [13 (13.27%)]. Simultaneous lung and liver CE were found in 11 cases (11.22%), and in 6 patients (6.12%), they were recognized in the abdominal cavity. The other locations of the hydatid cyst in CE cases are presented in Table 4. Accordingly, our findings conform to those reported in previous studies (28,29).
In this study, the age range of the patients was 8-91 years, with the highest rate in women of 21-30 (14.29%) and men of 31-40 and 41-50 years old (10.2%). Our findings are in agreement with those of Fallah et al (19), Yang et al (30), and Kebede et al (31). It seems that the establishment of infestation occurs even in younger age groups. Hence, improving health literacy via educational programs should focus on the mentioned age groups even younger as the main target populations.
It has already been assumed the liver is the first preferred immunological organ for CE and induces immune tolerance responses (32). Additionally, given that CE has a high affinity for the liver, patients permanently suffer from complications such as liver function disorders and changed metabolic health profiles, particularly liver enzymes (33). Furthermore, CE causes a significant burden of disease (32) among vulnerable populations. In addition, disability-adjusted life years (DALYs) is considered one of the most crucial subsequences of human hydatidosis (34). DALY has been estimated as 1210.12 years (YLD equals 177.12 and YLL equals 1033) in 2018 in Iran (34). Additionally, the highest amount of DALY in males and females were in the age groups of 45-59 and 30-44 years, respectively (34). In our study, the highest infection rate was significantly described in the liver (60.2%, P ≤ 0.05). Considerably, the other important point in our results was the significant parasitic age trend; it seems that disabilities as a serious concern would lead to long-term life which has a direct impact on increasing YLL.
In the present study, there was no relationship between age and involve organs (P = 0.079, Table 4). Although some parasites such as Coenurus cerebralis migrate through specific tissues which have evolved by the age trend, in accordance with our research, parasite migration to target tissues has not been supported via age trend, and the liver as the main target organ is at the same risk for all ages.
According to our research, the gradient percentage of infection has been reducing from 2014 to 2017, whilethe frequency significantly increased in 2018 (Figure 1) which was mainly due to infection reports relating to Malayer (11 cases), Nahavand (4 cases), and Tooviserkan (1 case) areas (Figure 2). The overall prevalence of CE cases in these areas was 61.53% in 2018 which were noticeable as a particular cultural and geographical zoon. However, the question is why the infection rate was significantly higher in Malayer compared to the other areas. In this regard, some fundamental points should be taken into consideration. Firstly, increasing the education level and public awareness assists in identifying the patients and leading them to medical centers in Hamedan. Secondly, the efficiency of parasitological diagnostic techniques and healthcare tests has been promoted. In other words, inappropriate healthcare management, increasing risk factors, and probable transmission methods can be effective. Thus, it is necessary to perform some hygienic practices, as well as preventive and treatment strategies, and increase public health knowledge in this respect.
Conclusion
According to the results, it seems that the targeted health education should focus on people in their third decade of life and younger. Secondly, the education of urban residents should focus more on the health of vegetables and villagers based on the parasite life cycle and simultaneous explanation of the dangers of contaminated vegetables and/or dogs. Hydatidosis is a public health concern in this area, and further epidemiological surveys are necessary to demonstrate the economic burden, risk factors, target populations, and control of the disease.
Acknowledgments
This study was a part of Master’s thesis number 2824006, approved by the Faculty of Veterinary Medicine, Bu-Ali Sina University, Hamedan, Iran. The authors appreciate the managers of hospitals for their sincere cooperation.
Authors’ Contribution
Conceptualization: Zainab Sadeghi Dehkordi.
Data curation: Zainab Sadeghi Dehkord.
Formal analysis: Ali Sadeghi-Nasab.
Funding acquisition: Zainab Sadeghi Dehkordi.
Investigation: Hamidreza Moslemomanesh.
Methodology: Zainab Sadeghi Dehkordi.
Project administration: Zainab Sadeghi Dehkordi.
Resources: Zainab Sadeghi Dehkordi.
Supervision: Zainab Sadeghi Dehkordi.
Validation: Zainab Sadeghi Dehkordi, Ali Sadeghi-Nasab.
Visualization: Zainab Sadeghi Dehkordi.
Writing–original draft: Zainab Sadeghi Dehkordi.
Writing–review & editing: Zainab Sadeghi Dehkordi, Ali Sadeghi-Nasab.
Competing Interests
The authors declare no conflict of interests.
Ethical Approval
this article is a part of Msc student thesis with 2601982 code which has been approved at Bu-Ali Sina university.
References
- Moradi M, Rampisheh Z, Roozbehani M, Razmjou E. A retrospective study of hydatid cysts in patients undergoing liver and lung surgery in Tehran, Iran. Heliyon 2019; 5(6):e01897. doi: 10.1016/j.heliyon.2019.e01897 [Crossref] [ Google Scholar]
- Ghorbanipour M, Sadeghi Dehkordi Z, Sazmand A, Daraei Garmakhany A, Fallah M, Sari AA. Optimizing the extraction conditions (solvent concentration and extraction time) of aqueous, alcoholic and hydroalcoholic extracts of Echinophoraplatyloba: antioxidant properties and its lethal effect on hydatid cyst protoscolex in laboratory condition. J Food Sci Technol 2023; 19(132):313-26. doi: 10.22034/fsct.19.132.313.[Persian] [Crossref] [ Google Scholar]
- Sadeghi Dehkordi Z, Eslami A. Parasitic Diseases in Dogs and Cats in Iran. Bu-Ali Sina University Publication; 2023. p. 91-7. [Persian].
- Panahi S. A report of a large hydatid cyst in the brain in 1369 in Tabriz. Tabriz Univ Med Sci 1995;24(9):3-8. [Persian].
- Jodti A, Yusef Nia MA, Tabatabai SMB. Report of two interesting and rare cases of hydatid cyst of the heart. Tabriz Univ Med Sci 2003;54:67-70. [Persian].
- Kitabchi SA, Qudsi SM. Report of two cases of spinal hydatid cyst. Med J Islam Repub Iran 2003;10(3):136-9. [Persian].
- Mahmoudi S, Karamet F. Report a case of breast hydatid cyst. Avicenna J Clin Med 2001;7(1):49-51. [Persian].
- Kamkarpour A, Libai E, Rozitalab H. Report of eye hydatid cyst. Bina 1997;6(2):166-8. [Persian].
- Sharifi N, Ghafarzadegan K. Hydatidosis: a rare case of bilateral tubo ovarian hydatid cyst. J Gorgan Univ Med Sci 2002;4(2):60-5. [Persian].
- Abedinzadeh A. Report of a rare case of hydatid cyst in the parathyroid gland. Iranian Ear, Throat, Nose and Throat Journal 1994;11(5):48-50. [Persian].
- Amouian S, Tayebi M, Mohamadian Roshan N. A retrospective study of 1759 cases of hydatid cyst in Mashhad university hospitals. Hakim Health Syst Res 2005;4(7):7-13. [Persian].
- Arbabi M, Houshyar H. Survey of echinococcosis and hydatidosis in Kashan region, central Iran. Iran J Public Health 2006; 35(1):75-81. [ Google Scholar]
- Davami MH, Fatahi Bayat F. An investigation on hydatid cysts which have surgically treated in Markazi province (Arak). J Arak Uni Med Sci 1997;1(5):12-5. [Persian].
- Sarkari B, Sadjjadi SM, Beheshtian MM, Aghaee M, Sedaghat F. Human cystic echinococcosis in Yasuj district in Southwest of Iran: an epidemiological study of seroprevalence and surgical cases over a ten-year period. Zoonoses Public Health 2010; 57(2):146-50. doi: 10.1111/j.1863-2378.2008.01200.x [Crossref] [ Google Scholar]
- Ghaffari S. Study of operated hydatid cysts cases in three medical centers of Babol medical university during 1991-96. J Babol Univ Med Sci 1999;1(1):27-33. [Persian].
- Shir Yazdi SM, Mir Shamsi MH, Hosseini B, Ebadi M. Cases of the hydatid cyst that were operated upon in Yazd. J Shahid Sadoughi Univ Med Sci 2000;1(8):25-30. [Persian].
- Gholami S, Tanzifi A, Sharif M, Daryani A, Rahimi MT, Mirshafiee S. Demographic aspects of human hydatidosis in Iranian general population based on serology: a systematic review and meta-analysis. Vet World 2018; 11(10):1385-96. doi: 10.14202/vetworld.2018.1385-1396 [Crossref] [ Google Scholar]
- Rokni MB. Echinococcosis/hydatidosis in Iran. Iran J Parasitol 2009; 4(2):1-16. [ Google Scholar]
- Fallah N, Rahmati K, Fallah M. Prevalence of human hydatidosis based on hospital records in Hamadan west of Iran from 2006 to 2013. Iran J Parasitol 2017; 12(3):453-60. [ Google Scholar]
- Sadeghi Dehkordi Z, Haseli R, Moeini B, Sazmand A. Assessment of knowledge, attitudes, and practices relating to parasitic diseases among pet owners in Hamadan and Kermanshah, Iran, from 2018 to 2020. J Ilam Univ Med Sci 2023;31(2):55-64. [Persian].
- Arbabi A, Masoud J. Seroepidemiological study in Hamedan province by IFA [thesis]. Tehran: School of Public Health, Tehran University; 1992. [Persian].
- Sadeghi Dehkordi Z, Sari AA, Panahi Z, Yalameha B. Parasitic contamination in raw vegetables and effect of washing procedure in Hamedan, Iran. Arch Hyg Sci 2019; 8(1):66-70. doi: 10.29252/ArchHygSci.8.1.66 [Crossref] [ Google Scholar]
- Salehi M, Adinezade A, Khodajou R, Saberi Karimian Z, Yousefi A. The epidemiologic survey of operated patients with hydatid cyst in hospitals of North Khorasan province during 2010-2011. J North Khorasan Uni Med Sci 2013; 4(4):623-9. doi: 10.29252/jnkums.4.4.623.[Persian] [Crossref] [ Google Scholar]
- Larrieu EJ, Costa MT, del Carpio M, Moguillansky S, Bianchi G, Yadon ZE. A case-control study of the risk factors for cystic echinococcosis among the children of Rio Negro province, Argentina. Ann Trop Med Parasitol 2002; 96(1):43-52. doi: 10.1179/000349802125000501 [Crossref] [ Google Scholar]
- Wang Q, Qiu JM, Schantz P, He JG, Ito A, Liu FJ. Investigation of risk factors for development of human hydatidosis among households raising livestock in Tibetan areas of western Sichuan province. Zhongguo Ji Sheng Chong Xue Yu Ji Sheng Chong Bing Za Zhi 2001; 19(2):93-6. [ Google Scholar]
- Ghabouli Mehrabani N, Kousha A, Khalili M, Mahami Oskouei M, Mohammadzadeh M, Alizadeh S. Hydatid cyst surgeries in patients referred to hospitals in East Azerbaijan province during 2009-2011. Iran J Parasitol 2014; 9(2):233-8. [ Google Scholar]
- McManus DP. Echinococcosis with particular reference to Southeast Asia. Adv Parasitol 2010; 72:267-303. doi: 10.1016/s0065-308x(10)72010-8 [Crossref] [ Google Scholar]
- Hamzavi Y, Vejdani M, Nazari N, Mikaeili A. The trend of hydatidosis in Kermanshah province, western Iran (1986-2008). Iran J Parasitol 2011; 6(4):33-40. [ Google Scholar]
- Kohansal MH, Nourian A, Bafandeh S. Human cystic echinococcosis in Zanjan area, northwest Iran: a retrospective hospital based survey between 2007 and 2013. Iran J Public Health 2015; 44(9):1277-82. [ Google Scholar]
- Yang YR, Cheng L, Yang SK, Pan X, Sun T, Li X. A hospital-based retrospective survey of human cystic and alveolar echinococcosis in Ningxia Hui Autonomous Region, PR China. Acta Trop 2006; 97(3):284-91. doi: 10.1016/j.actatropica.2005.12.001 [Crossref] [ Google Scholar]
- Kebede N, Mitiku A, Tilahun G. Retrospective survey of human hydatidosis in Bahir Dar, north-western Ethiopia. East Mediterr Health J 2010; 16(9):937-41. [ Google Scholar]
- Peters L, Burkert S, Grüner B. Parasites of the liver–epidemiology, diagnosis and clinical management in the European context. J Hepatol 2021; 75(1):202-18. doi: 10.1016/j.jhep.2021.02.015 [Crossref] [ Google Scholar]
- Rahimi M, Kheiandish F, Arab-Mazar Z, Mirzapour A. Level of liver enzymes in patients with mono-parasitic infections. Infect Epidemiol Microbiol 2017; 3(4):137-42. doi: 10.18869/modares.iem.3.4.137 [Crossref] [ Google Scholar]
- Parandin F, Heydarpour F, Mohebali M, Hanafi-Bojd AA, Akbari Sari A, Zeynali M. Estimation of burden of cystic echinococcosis in Iran using disability adjusted life years (DALYs) in 2018. Iran J Public Health 2021; 50(11):2302-8. doi: 10.18502/ijph.v50i11.7586 [Crossref] [ Google Scholar]